Category: Parkinsonism, Atypical: PSP, CBD
Objective: To evaluate the validity and precision of using inertial measurement units (IMU) for measurement of kinematics and spatial-temporal features of gait in progressive supranuclear palsy (PSP).
Background: PSP is a neurodegenerative tauopathy characterized by prominent gait and balance impairment. Quantified gait analysis allows for objective measurement of these deficits. Lab-based three-dimensional video motion capture (mocap) is highly accurate, but resource intensive, while IMUs offer an accessible alternative. IMUs have been shown to perform well in normal individuals and Parkinson’s disease [1,2].
Method: Patients who met the 2017 MDS criteria for PSP were recruited for gait analysis. Mocap was performed using a 52-marker modified Helen-Hayes system. Simultaneously, six IMUs were affixed to the body using double-sided tape (sternum, sacrum, bilateral wrists, and feet). Participants walked at a self-selected pace on a 10-meter walkway for 3 trials. Spatial-temporal features (velocity and stride length) and kinematics (trunk and pelvis range of motion (ROM) in frontal, sagittal, and transverse planes) were calculated and compared for both modalities, with mocap as gold-standard. Bland-Altman plots and limit of agreement (LoA) were used to assess accuracy. Root mean squared error (RMSE) was used to assess precision.
Results: A total of 17 (6 female) participants were assessed (age 70±10 years, height 167±8 cm, PSP rating scale 27±10). Accuracy: IMU measurements for velocity and stride length were larger than mocap measurements. Mean difference for velocity was 7.66 cm/s (-5.85-21.17) [figure1] and for stride length was 9.21 cm (-2.53-20.95) [figure2]. The trunk and pelvis ROM measured by IMU was within 6-7 degrees of mocap [figure3]. Precision: For both mocap and IMU, ROM measurements were within 5 degrees. Mocap RMSE values for velocity (1.19-10.64 cm/s) and stride length (0.87-8.56 cm) were slightly larger than IMU values for velocity (1.32-9.25 cm/s) and stride length (0.87-6.64 cm).
Conclusion: IMU demonstrated good agreement with mocap for ROM measurement in PSP. Spatial-temporal measurements were higher for IMUs than mocap, with wider range of error either due to disease heterogeneity or device performance in this setting. Device accuracy and precision should be evaluated prior to clinical or research application.
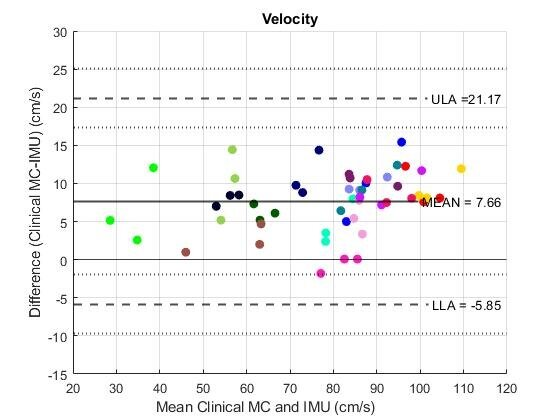
Figure 1
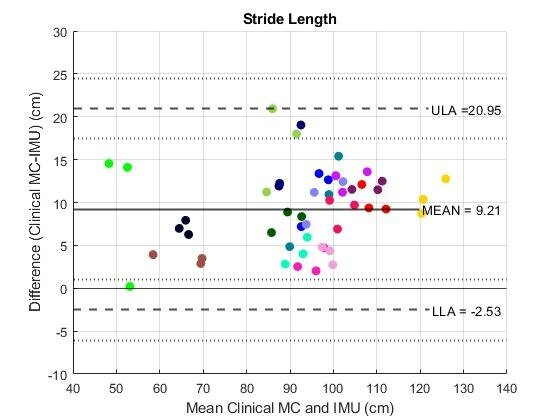
Figure 2
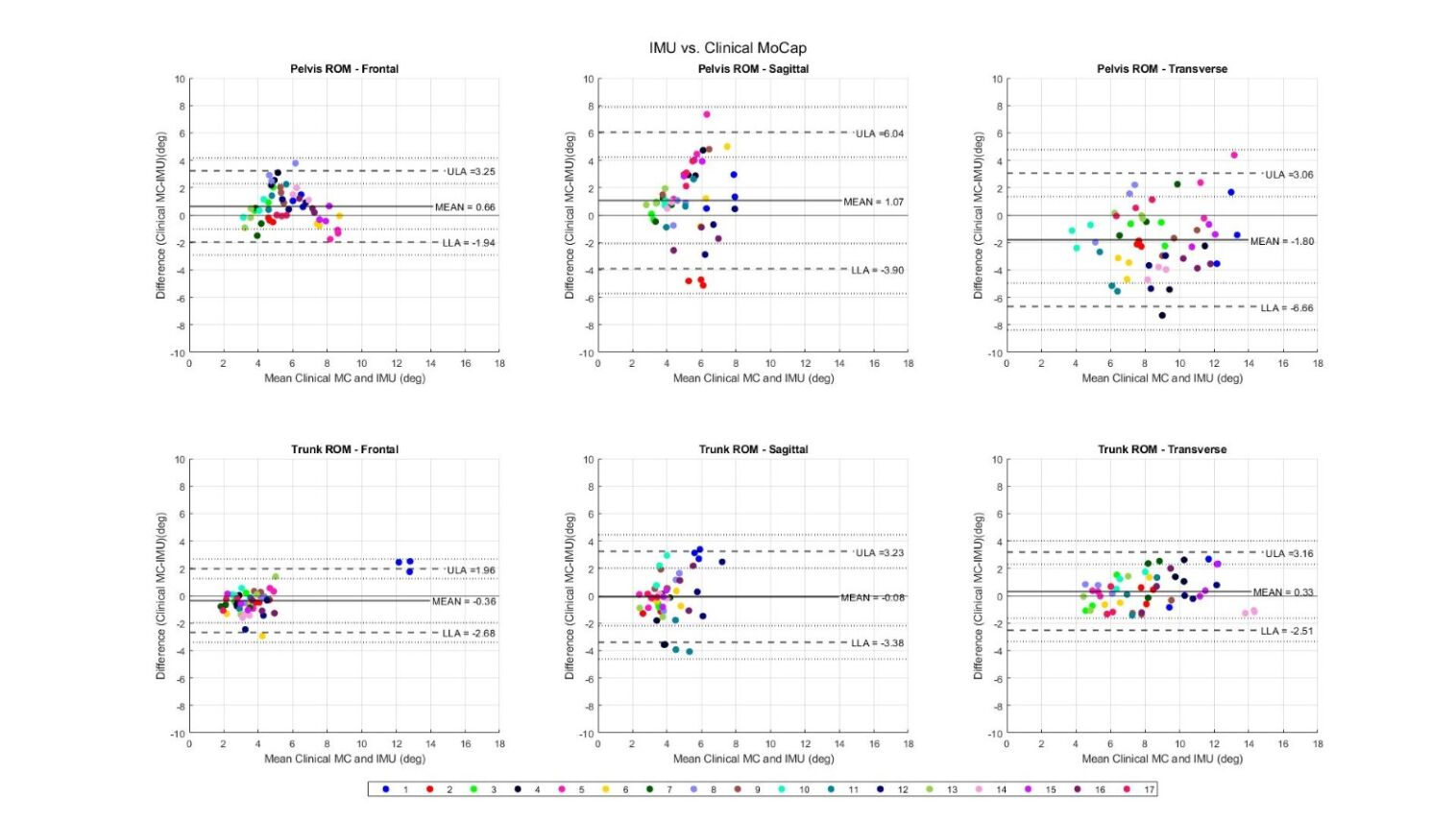
Figure 3
References: [1] Hori K, Mao Y, Ono Y, Ora H, Hirobe Y, Sawada H, Inaba A, Orimo S, Miyake Y. Inertial Measurement Unit-Based Estimation of Foot Trajectory for Clinical Gait Analysis. Front Physiol. 2020 Jan 10;10:1530. doi: 10.3389/fphys.2019.01530. PMID: 31998138; PMCID: PMC6966410.
[2] Mancini M, Horak FB. Potential of APDM mobility lab for the monitoring of the progression of Parkinson’s disease. Expert Rev Med Devices. 2016 May;13(5):455-62. doi: 10.1586/17434440.2016.1153421. PMID: 26872510; PMCID: PMC4959602.
To cite this abstract in AMA style:
A. Blazek, C. Hogen, J. Whitwell, K. Josephs, K. Kaufman, F. Ali. Validation of Inertial Monitoring Units for Gait Assessment in Progressive Supranuclear Palsy [abstract]. Mov Disord. 2024; 39 (suppl 1). https://www.mdsabstracts.org/abstract/validation-of-inertial-monitoring-units-for-gait-assessment-in-progressive-supranuclear-palsy/. Accessed May 7, 2026.« Back to 2024 International Congress
MDS Abstracts - https://www.mdsabstracts.org/abstract/validation-of-inertial-monitoring-units-for-gait-assessment-in-progressive-supranuclear-palsy/