Category: Choreas (Non-Huntington's Disease)
Objective: Nonketotic hyperglycemia (NKH), also known as Diabetic Striatopathy (DS) can present with different involuntary movements in diabetic patients. Hemichorea-hemiballismus (HC-HB) is the most common abnormal movement, but occasionally Hemifacial Spasm (HFS) is also reported in rare instances. We here report one such interesting case, where Hemichorea-Hemiballismus-Hemifacial Spasm (HC-HB-HFS) was seen together in an elderly diabetic lady.
Background: NA
Method: An 89-year-old lady presented in the neurology clinic with a 10-day history of right upper and lower limb abnormal repetitive and flinging movements suggesting HC-HB, along with right hemifacial spasm (HFS). She was evaluated for this in a nearby hospital, and found to have high blood sugars (410 mg/dl), She was started on anti-diabetic treatment and referred to a higher centre. On evaluation, she had HC-HB-HFS, without any motor, sensory or cerebellar involvement. In our hospital, her blood sugar was 345 mg/dl with HBA1C of 9.2. Arterial blood gas analysis showed normal pH, bicarbonates, serum osmolarity and electrolytes. MRI Brain showed T-1 hyperintense signals in the left putamen suggesting diabetic striatopathy causing HC-HB-HFS (Figure 1). The patient was started on subcutaneous insulin and benzodiazepines (clonazepam 0.25 mg three times a day). The patient started showing improvement, the first to improve was HFS, and then her choreo-ballistic movements subsided over 7-10 days.
Results: Though the pathophysiological mechanisms of HC-HB and HFS are different, both have been reported in diabetic patients. Hyperglycemia-associated perturbations in inhibitory neurotransmitters and ischemic damage to basal ganglia structures are possible causes for HC-HB, but HFS is possibly caused due to hyperglycemia-associated facial nerve ischemic or vascular damage. Fortunately, with the improvement of the glycemic status of patients, these movement disorders reverse, as in our patient, suggesting a temporary nature of impairment caused by NKH.
Conclusion: The occurrence of HC-HB-HFS together in DS/NKH is unusual and possibly not reported earlier. However, it’s important to recognize and treat these acute onset movement disorders associated with poor glycemic status of patients as they are reversible if treated timely.
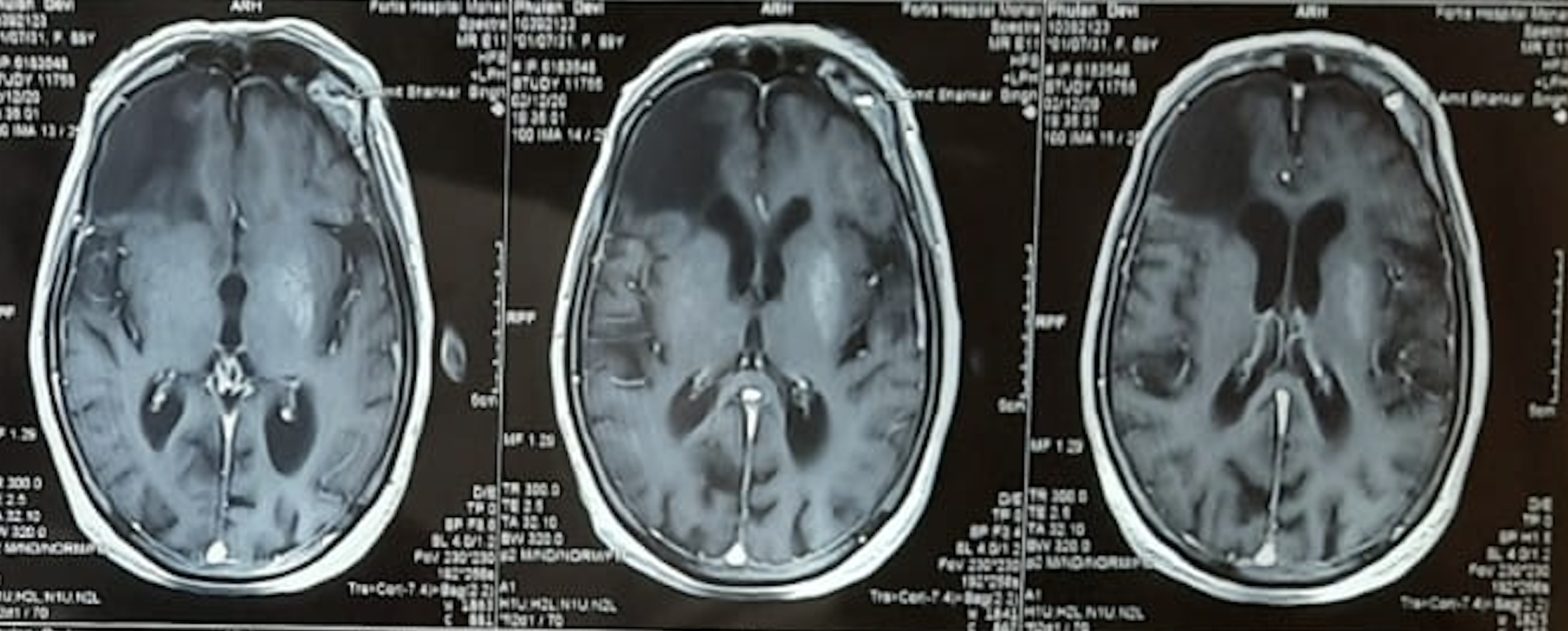
MRI T1 with Hyperintense Signal in left putamen
To cite this abstract in AMA style:
D. Das, A. Singh, J. Singhvi. Reversible Hemichorea-Hemiballismus-Hemifacial Spasm in Diabetic Striatopathy [abstract]. Mov Disord. 2024; 39 (suppl 1). https://www.mdsabstracts.org/abstract/reversible-hemichorea-hemiballismus-hemifacial-spasm-in-diabetic-striatopathy/. Accessed April 18, 2025.« Back to 2024 International Congress
MDS Abstracts - https://www.mdsabstracts.org/abstract/reversible-hemichorea-hemiballismus-hemifacial-spasm-in-diabetic-striatopathy/