Session Information
Date: Monday, June 5, 2017
Session Title: Parkinsonism, MSA, PSP (Secondary and Parkinsonism-Plus)
Session Time: 1:45pm-3:15pm
Location: Exhibit Hall C
Objective: Clinical description of a patient with familial FTD with a rapidly progressive parkinsonism.
Background: FTD typically presents with behavioral and cognitive deficits, but extrapyramidal symptoms are also common. The pathophysiologic basis of these symptoms is unclear and generally had a poor response to dopaminergic replacement therapies. The results of dopaminergic imaging in patients with FTD in literature are controversial, and even less information is available in the cases of familial FTD.
Methods: A 81 years-old male patient, developed at age of 75, cognitive deficits characterized initially by obsessive behaviors, irritability and aggressive behaviors. His symptoms progressively worsened and at age of 80, he has lost functional autonomy and was institutionalized. At age 81, he displayed for the first time an asymmetrical akinetic-rigid syndrome, and treatment with levodopa/carbidopa was started, with poor clinical benefit. He presented in neuropsychological assessment a MoCA of 16 and FAB of 14(7 years of education). In neurological examination, he presented symmetric apraxia, asymmetrical akinetic-rigid syndrome (more prominent in the left side), moderate loss of postural reflexes, freezing of gait and parkinsonian gait (MDS-UPDRS-III:72;H&Y:4). 8 months after the beginning of extrapyramidal symptoms he loss gait autonomy and was bedridden. The patient’s mother and sister presented a similar clinical picture with behavioral symptoms beginning at age of 70’s, and with a rapid progressive asymmetric parkinsonism.
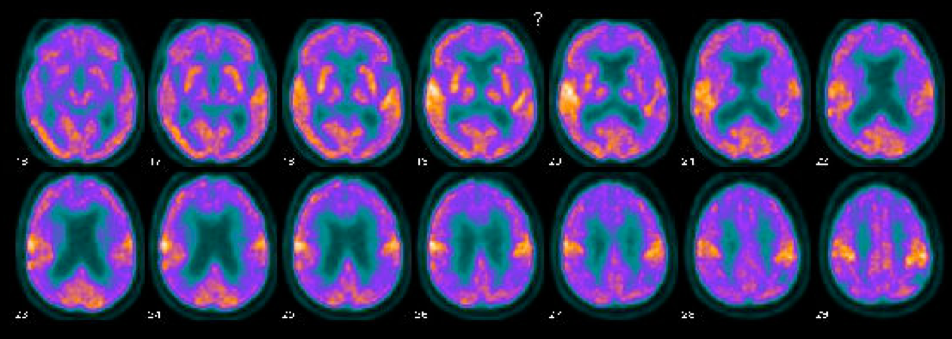
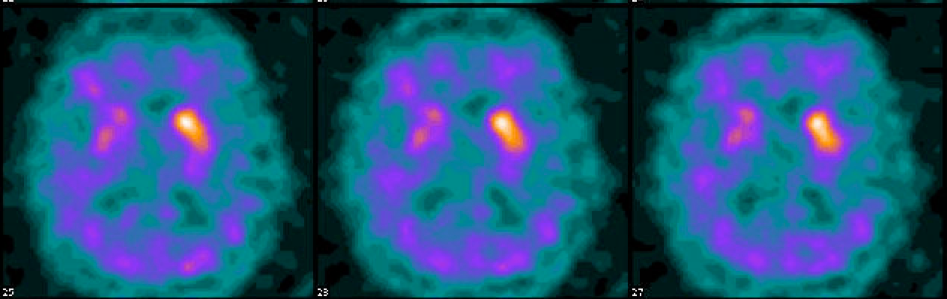
Results: Brain MRI demonstrated generalized brain atrophy, slightly asymmetrical (more prominent in left hemisphere), and more obvious in fronto-temporal regions. DATSCAN revealed markedly asymmetric bilateral dopaminergic deficit, more prominent in right side [Figure 1]. FDG-PET showed frontal, temporal and parietal hypometabolism (slight left hemisphere predominance) [Figure 2]. CSF biomarkers showed marked increase in Tau and p-Tau with normal beta-amyloid levels. Results of genetic test will be presented.
Conclusions: This case describes a case of familial FTD with autosomal dominant pattern of transmission with evidence of dopaminergic deficit markedly asymmetrical in DATSCAN. Furthermore, highlights the importance of dopaminergic imaging in this cases to guide not only diagnosis but also management, due the implications that dopaminergic therapies can have on behavioral symptoms.
To cite this abstract in AMA style:
M. Sousa, R. Varela, C. Januário, A. Morgadinho. Pre-synaptic dopaminergic deficit in a patient with familial FTD [abstract]. Mov Disord. 2017; 32 (suppl 2). https://www.mdsabstracts.org/abstract/pre-synaptic-dopaminergic-deficit-in-a-patient-with-familial-ftd/. Accessed April 20, 2025.« Back to 2017 International Congress
MDS Abstracts - https://www.mdsabstracts.org/abstract/pre-synaptic-dopaminergic-deficit-in-a-patient-with-familial-ftd/