Objective: To demonstrate the feasibility of non-staged intraoperative MRI (iMRI) deep brain stimulation (DBS) lead revision under general anesthesia (GA).
Background: DBS lead revision surgery due to therapy failure from suboptimal lead positioning is common, making up approximately 30% of the cases. Lead revisions are often performed awake with microelectrode recording. However, there is no standard guideline and lead revision practices vary among centers. iMRI-guided DBS lead implantation under GA is gaining popularity and is associated with good targeting accuracy and clinical outcomes. Here, we present a cervical dystonia patient who successful underwent MRI-guided bilateral GPi DBS lead revision under GA, during which we performed concurrent new lead implantation and old lead removal. iMRI helps identify optimal entry points and trajectories, and tracts both brain shift and lead position in real-time, thereby potentially reducing the need for staged revision surgeries.
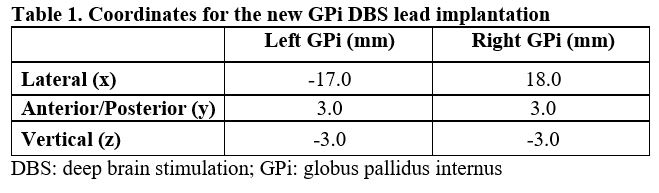
Method: A 60-year-old woman with refractory adult-onset isolated cervical dystonia underwent awake, frame-based microelectrode-recording (MER) guided bilateral GPi DBS implantation. She initially had a favorable response but lost therapeutic benefit after 2 years. Side-effect (SE) profile suggested lateral lead placement, which was confirmed with MRI. Bilateral lead revision surgery was recommended due to symptom progression and limited reprogramming options due to intolerable SEs within the therapeutic range. iMRI-guided surgery under GA was planned due to her hyperkinetic symptoms and patient preference. Using a 1.5T iMRI and iMRI compatible stereotactic system, new trajectories were designed to target the GPis without crossing the existing leads (Left x:-17.0mm, y:3.0mm, z:3.0mm; Right x:18.0mm, y:3.0mm, z:-3.0mm). New leads were placed through the existing burr holes, into the new targets with radial errors <0.08mm. Old leads were removed next, and the new leads were connected to the existing implantable pulse generator.
Results: The patient tolerated the procedure well. The new leads were medial to the old leads (Left 2mm; Right 6mm) and she had measurably improved side-effect profile at all contacts at 1-month follow-up.
Conclusion: Non-staged iMRI-guided DBS lead revision is technically feasible and is an alternative strategy to staged iMRI-guided or awake MER-guided revision surgeries, particularly in patients with claustrophobia or hyperkinetic movement disorders.
References: [1] Rolston JD, Englot DJ, Starr PA, Larson PS. An unexpectedly high rate of revisions and removals in deep brain stimulation surgery: Analysis of multiple databases. Parkinsonism Relat Disord. 2016;33: 72-77. https://doi.org/10.1016/j.parkreldis.2016.09.014. [2] Sharma VD, Bezchlibnyk YB, Isbaine F, et al. Clinical outcomes of pallidal deep brain stimulation for dystonia implanted using intraoperative MRI. J Neurosurg. 2019: 1-13. https://doi.org/10.3171/2019.6.JNS19548. [3] Falowski SM, Bakay RA. Revision Surgery of Deep Brain Stimulation Leads. Neuromodulation. 2016;19(5): 443-450. https://doi.org/10.1111/ner.12404.5. [4] Frizon LA, Nagel SJ, May FJ, et al. Outcomes following deep brain stimulation lead revision or reimplantation for Parkinson’s disease. J Neurosurg. 2018: 1-6. https://doi.org/10.3171/2018.1.JNS171660. https://doi.org/10.1227/01.NEU.0000325492.58799.35. [5] Richardson RM, Ostrem JL, Starr PA. Surgical repositioning of misplaced subthalamic electrodes in Parkinson’s disease: location of effective and ineffective leads. Stereotact Funct Neurosurg. 2009;87(5): 297-303. https://doi.org/10.1159/000230692.
To cite this abstract in AMA style:
B. Hwang, D. Mampre, K. Mills, A. Butala, W. Anderson. Non-Staged Bilateral GPi DBS Lead Revision Using iMRI: A Case Report [abstract]. Mov Disord. 2020; 35 (suppl 1). https://www.mdsabstracts.org/abstract/non-staged-bilateral-gpi-dbs-lead-revision-using-imri-a-case-report/. Accessed June 20, 2026.« Back to MDS Virtual Congress 2020
MDS Abstracts - https://www.mdsabstracts.org/abstract/non-staged-bilateral-gpi-dbs-lead-revision-using-imri-a-case-report/