Category: Choreas (Non-Huntington's Disease)
Objective: Illustrate two cases of late-onset chorea attributable to cerebrovascular disease
Background: “Senile chorea” has been used to describe late-onset (age 50+), sporadic, hyperkinetic movements. Most neurologists contest this diagnosis, as many cases have a known, treatable cause. [1] We suggest that cerebral small vessel ischemia may be an underrecognized cause of chorea in patients with a negative diagnostic evaluation.
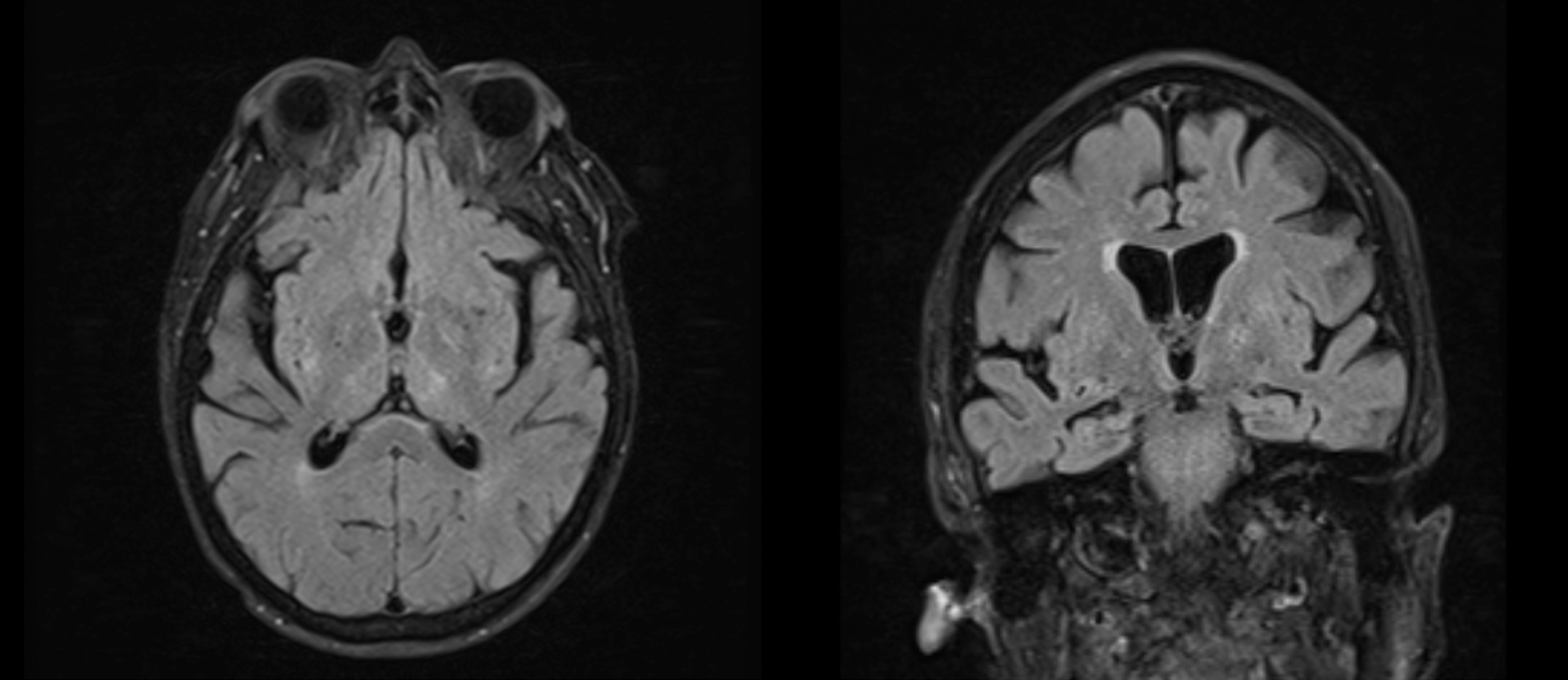
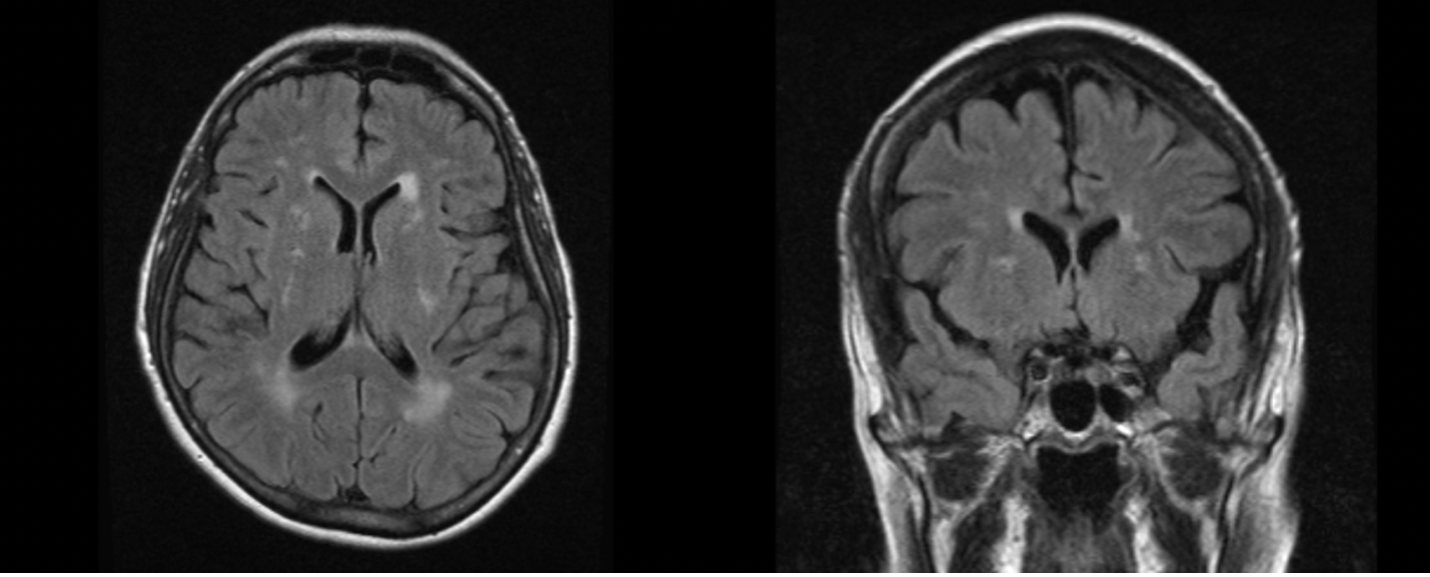
Method: Patient 1 is an 81-year-old female with neurovascular risk factors who presented with 4 years of worsening, unbothersome movements of the head and extremities. Exam showed mild, continuous choreiform movements of the neck, face, bilateral hands and feet at rest. Movements improved with action but could not be voluntarily suppressed. There was no motor impersistence of tongue protrusion. Workup was negative for secondary causes of chorea, however MRI brain was notable for chronic small vessel disease in the bilateral basal ganglia and left thalamus [figure1]. Patient 2 is a 67-year-old woman who presented with 5 years of insuppressible, unbothersome movements of the upper and lower extremities. Exam was notable for mild, continuous generalized chorea, involving more upper than lower extremities. Milkmaid’s grip was present without motor impersistence of tongue protrusion. Workup was negative for secondary causes of chorea, however MRI brain showed scattered FLAIR changes in the basal ganglia, pons, centrum semiovale, and corona radiata consistent with chronic small vessel disease [figure2].
Results: There are few cases of sporadic, late-onset chorea in the literature. However, most tend to be over the age of 50, as seen in our cases. [2] In both cases, patient was unaware of their symptoms, unlike those with a primary neurodegenerative disorder, such as Huntington’s. Bloodwork for known causes of chorea were negative. MRI may not always show discrete lesions as the infarcts may be too small.
Conclusion: These cases illustrate that generalized small vessel disease may be an undiagnosed cause of late onset chorea. MRI is supportive of vascular chorea if the lesions are in bilateral globus pallidus, substantia nigra, or thalamus. This may be suspected in patients with vascular risk factors such as hypertension, hyperlipidemia, diabetes, smoking, or obesity, but does not preclude workup for other causes of chorea. As these patients are at continued risk for vascular injury, it is prudent to control risk factors.
References: [1] Warren JD, Firgaira F, Thompson EM, Kneebone CS, Blumbergs PC, Thompson PD. The causes of sporadic and ‘senile’ chorea. Australian and New Zealand Journal of Medicine. 1998;28(4):429-431. [2] Piccolo I, Defanti CA, Soliveri P, Volontè MA, Cislaghi G, Girotti F. Cause and course in a series of patients with sporadic chorea. J Neurol. 2003;250(4):429-435.
To cite this abstract in AMA style:
C. Selvadurai, A. Patel. Late-onset chorea in the setting of cerebrovascular disease [abstract]. Mov Disord. 2021; 36 (suppl 1). https://www.mdsabstracts.org/abstract/late-onset-chorea-in-the-setting-of-cerebrovascular-disease/. Accessed May 15, 2026.« Back to MDS Virtual Congress 2021
MDS Abstracts - https://www.mdsabstracts.org/abstract/late-onset-chorea-in-the-setting-of-cerebrovascular-disease/