Category: Pediatric Movement Disorders
Objective: We aim to explore motor control in children with essential tremor (ET) utilizing the Kinarm exoskeleton robot.
Background: Tremor is one of the most common movement disorders during childhood. Quantification of kinematic motor deficits in a reaching task may advance our understanding of pathophysiology and treatment opportunities.
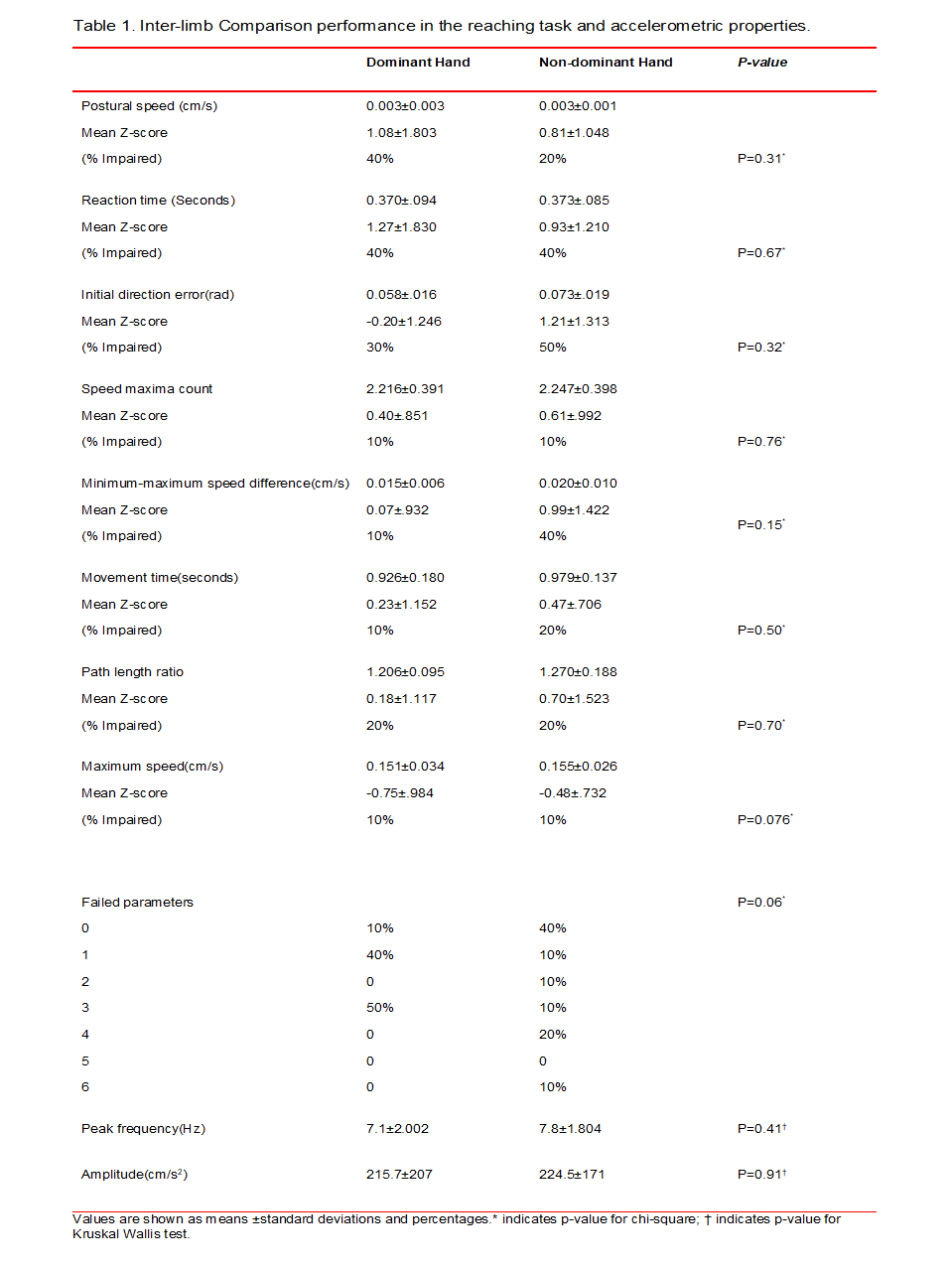
Method: We report preliminary data from ten pediatric patients with ET. Clinical evaluation was performed with the Tremor Rating Scale (TRS). Tremor activity was measured using triaxial accelerometers placed equidistantly at the dorsum of the hands and arms; the signal was analyzed using principal component analysis and Fast Fourier Transform, in order to measure the dominant peak frequency of tremor, and tremor power between 0-30 hertz band. Kinematic evaluation was conducted with a validated reaching task protocol from the Kinarm exoskeleton. The robot yields 8 different parameters from the reaching movements, which were subsequently converted to normalized Z-scores based on a sample of 155 normal controls.
Results: Mean age was 13.8 (SD 2.1) years, 70% were male. Mean age at onset of tremor was 9.3 (SD 5.3) years. Mean TRS score was 10.3 (SD 7.3). Postural tremor peak frequency of the dominant hand was 7.1 (SD 2.1) hz; mean amplitude 215.7 (SD 205.9) cm/s2. Non dominant hand mean frequency 7.8 (SD 1.8) hz; mean amplitude 224.5 (SD 167.7) cm/s2. With regards to the reaching task, half were impaired in 3 parameters in the dominant hand, and 40% showed deficits in 3 or more parameters with the nondominant hand. The most frequently affected parameters were reaction time (40%) and posture speed in the dominant hand (40%), whereas initial direction error (50%) and Minimum-maximum speed difference (50%) were the most commonly affected in the non dominant hand. The correlation coefficient between the number of impaired parameters in the reaching task and TRS score; number of impaired parameters and peak frequency; number of impaired parameters and amplitude revealed a positive trend; however, it did not reach statistical significance.
Conclusion: Our initial sample of children with ET show deficits within various aspects of motor control. Distinguishing and quantifying these features may serve as a marker of severity. Moreover, it may unveil intrinsic components and compensatory mechanisms in ET. A larger sample may demonstrate an association between motor control and clinical rating scales/accelerometric properties.
References: 1. Mochizuki G, Centen A, Resnick M, et al. Movement kinematics and proprioception in post-stroke spasticity: assessment using the Kinarm robotic exoskeleton. J Neuroeng Rehabil 2019; 16: 146. 2. Semrau JA, Herter TM, Scott SH, et al. Inter-rater reliability of kinesthetic measurements with the KINARM robotic exoskeleton. Journal of NeuroEngineering and Rehabilitation; 14. Epub ahead of print 2017. DOI: 10.1186/s12984-017-0260-z. 3. Ghosh D, Brar H, Lhamu U, et al. A Series of 211 Children with Probable Essential Tremor. Mov Disord Clin Pract 2017; 4: 231–236.
To cite this abstract in AMA style:
A. Medina Escobar, N. Cothros, R. Hawe, D. Martino, S. Dukelow, A. Kirton, E. Roze, E. Nosratmirshekarlou, T. Pringsheim. Kinematic control in children with essential tremor [abstract]. Mov Disord. 2020; 35 (suppl 1). https://www.mdsabstracts.org/abstract/kinematic-control-in-children-with-essential-tremor/. Accessed April 21, 2025.« Back to MDS Virtual Congress 2020
MDS Abstracts - https://www.mdsabstracts.org/abstract/kinematic-control-in-children-with-essential-tremor/