Session Information
Date: Monday, June 5, 2017
Session Title: Parkinsonism, MSA, PSP (Secondary and Parkinsonism-Plus)
Session Time: 1:45pm-3:15pm
Location: Exhibit Hall C
Objective: To compare differences in local dynamic stability (LDS) and its association with stride width in individuals with idiopathic Parkinson’s Disease (iPD), individuals with frontal gait disorders (FGD), and healthy elderly.
Background: LDS is often described as an indicator of the ability of the neuromuscular control system to attenuate local perturbations, and it is a sensitive predictor of fall risk in elderly adults. Despite the high rate of falls and gait disorders in individuals with iPD or FGD, the complex dynamics of gait such as LDS have not been well explored. In particular, it is unknown whether wider strides adopted by subjects with FGD, considered cautious and more statically stable than narrower strides, benefit LDS.
Methods: Thirty-eight subjects with iPD (69±12 yrs, MDS-UPDRS Part 3: 34±12), 17 subjects with FGD (73±7 yrs), and 24 healthy control subjects (71±8 yrs) participated. No subject with iPD reported freezing of gait on the NFOG-Q. Subjects with iPD or FGD were tested >12 hours after withholding anti-PD medication. Subjects walked overground at their comfortable pace for two minutes. Inertial sensors (APDM) on the sternum collected tri-axial accelerations and angular velocities at 128 Hz. Multiple bouts of 5 steady state strides were extracted and time-normalized. A 9D state space was constructed using the 3D accelerations and twice-time-delayed copies. LDS was estimated from the maximum finite-time Lyapunov exponent by taking the slope of the mean log divergence curve from 0 – 0.5 strides. Separately, participants walked across an 8 m GAITRite mat three times and the average stride width was extracted. ANOVA and Tukey post-hoc tests compared LDS and stride width across groups, and Pearson correlation coefficients compared LDS to stride width.
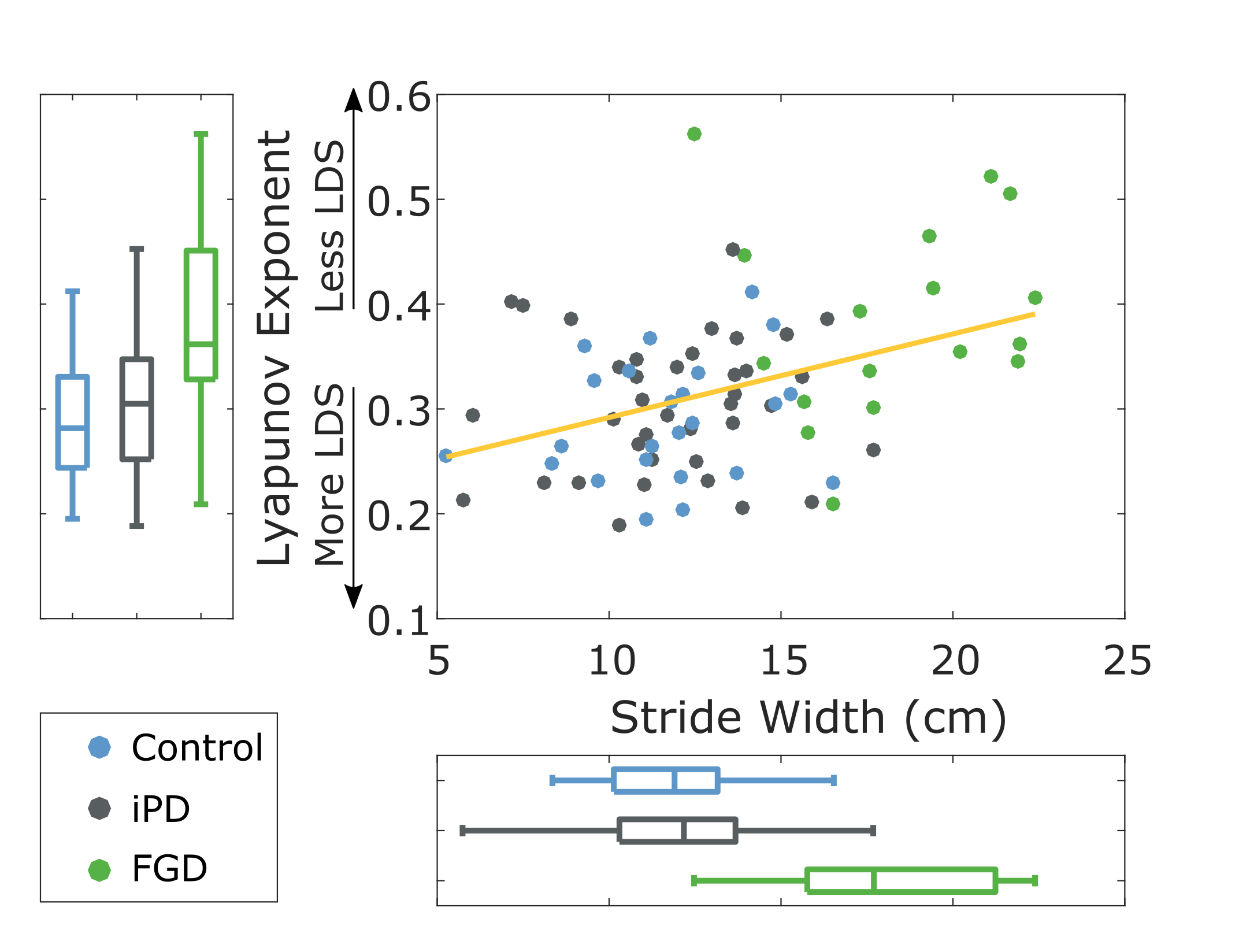
Results: Subjects with FGD had wider strides and worse LDS compared to subjects with iPD and controls (p <0.01). LDS did not differ between controls and subjects with iPD. Across all subjects, stride width was inversely correlated with LDS (r = 0.39, p <0.01) (Fig 1). [figure1]
Conclusions: Neurological dysfunction associated with FGD produces less stable dynamic control of the upper body during gait. The association between wider strides and less LDS suggests wider steps may adversely affect LDS, potentially caused by larger mediolateral velocity of the center-of-mass. Future studies should examine the relationship between preferred step width, LDS, and falls throughout disease progression.
References: Rispens, S. M., K. S. van Schooten, M. Pijnappels, A. Daffertshofer, P. J. Beek and J. H. van Dieën (2014). “Identification of fall risk predictors in daily life measurements gait characteristics’ reliability and association with self-reported fall history.” Neurorehabilitation and neural repair: 1545968314532031.
Young, P. M. M. and J. B. Dingwell (2012). “Voluntarily changing step length or step width affects dynamic stability of human walking.” Gait & posture 35(3): 472-477.
To cite this abstract in AMA style:
P. Fino, C. Curtze, M. Mancini, P. Carlson-Kuhta, J. Nutt, F. Horak. Dynamic Instability and Stride Width in Parkinsonism [abstract]. Mov Disord. 2017; 32 (suppl 2). https://www.mdsabstracts.org/abstract/dynamic-instability-and-stride-width-in-parkinsonism/. Accessed April 20, 2025.« Back to 2017 International Congress
MDS Abstracts - https://www.mdsabstracts.org/abstract/dynamic-instability-and-stride-width-in-parkinsonism/