Category: Surgical Therapy: Parkinson's Disease
Objective: To present a case with a severe life-threatening microlesion effect related with STN DBS rescued with a tractography-guided neuromodulation approach
Background: Microlesion effect have been described as a transient clinical improvement after lead penetration in the target area in patients undergoing deep brain stimulation. Severe persistent dyskinesia after DBS lead placement in the subthalamic nucleus have been rarely described2.
Method: We report a case of a 67-year-old woman diagnosed with PD fifteen years before the surgery. The levodopa-equivalent daily dose was 325 mg before surgery and the UPDRS OFF was 23 and ON was 0. She underwent DBS with directional leads in a staged fashion. After the right lead was implanted she was discharged home with no complications. Two days later the patient started with dyskinesias in the left hemibody (USCRS8item 16: 6). The first approach was to discontinue the levodopa and prescribe long-acting amantadine with no improvement. Three days later the dyskinesias worsened and the patient had to be admitted to the intensive care unit due to severe dyskinesias, rhabdomyolysis, and metabolic acidosis. We tetrabenazine with improvement of the dyskinesias but worsening of the Parkinsonism.
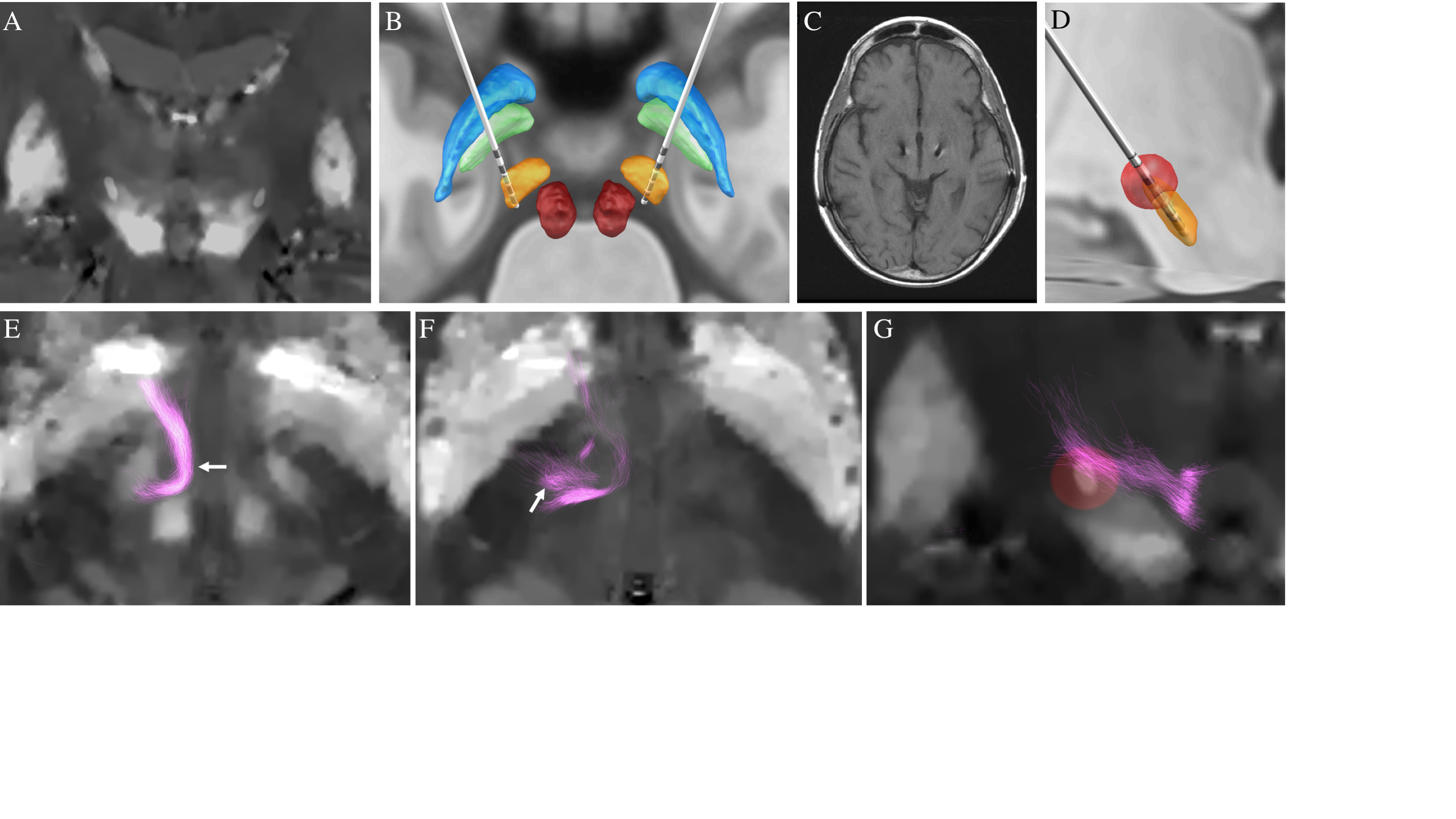
Results: We performed a tractography analysis to identify the pallidofugal pathways (Fig 1). The most dorsal (fourth) contact and the anteromedial/posterior segments of the third contact had direct access to this pathway. She underwent bilateral internal pulse generator implantation. Immediately after the surgery, we activated the fourth contact and the dyskinesias dramatically improved (USCRS 2). The improvement was optimized by adding the anteromedial and posterior segments of the third contact (settings: 4-3AB-C+, 90 µs, 130Hz) with total suppression of the rest dyskinesias and ~75% reduction of the action dyskinesias. Brief discontinuation of the stimulation resulted in a relapse of severe dyskinesias. Postoperative MRI of the brain did not show evidence of stroke or bleeding in the subthalamic area.
Conclusion: In summary, severe dyskinesias related with microlesion effect could be rescued with pallidofugal stimulation if the most dorsal contacts have access to this antidyskinetic circuit. This strategy may avoid the need to reimplant in the GPi area. Tractography can identify this pathway individually with good anatomical accuracy in a patient-specific manner.
References: 1. Gago MF, Rosas MJ, Linhares P, Ayres-Basto M, Sousa G, Vaz R. Transient disabling dyskinesias: a predictor of good outcome in subthalamic nucleus deep brain stimulation in Parkinson’s disease. Eur Neurol. 2009;61(2):94-99. doi:10.1159/000177941 2. Cook RJ, Jones L, Fracchia G, et al. Globus pallidus internus deep brain stimulation as rescue therapy for refractory dyskinesias following effective subthalamic nucleus stimulation. Stereotact Funct Neurosurg. 2015;93(1):25-29. doi:10.1159/000365223 3. Sriram A, Foote KD, Oyama G, Kwak J, Zeilman PR, Okun MS. Brittle Dyskinesia Following STN but not GPi Deep Brain Stimulation. Tremor and Other Hyperkinetic Movements. 2014;4:242. doi:10.5334/tohm.183 4. Ramirez-Zamora A, Ostrem JL. Globus Pallidus Interna or Subthalamic Nucleus Deep Brain Stimulation for Parkinson Disease. JAMA Neurol. 2018;75(3):367. doi:10.1001/jamaneurol.2017.4321 5. Herzog J, Pinsker M, Wasner M, et al. Stimulation of subthalamic fibre tracts reduces dyskinesias in STN-DBS. Mov Disord. 2007;22(5):679-684. doi:10.1002/mds.21387 6. Goftari M, Kim J, Johnson E, et al. Pallidothalamic tract activation predicts suppression of stimulation-induced dyskinesias in a case study of Parkinson’s disease. Brain Stimul. 2020;13(6):1821-1823. doi:10.1016/j.brs.2020.09.022 7. Katayama Y, Oshima H, Kano T, Kobayashi K, Fukaya C, Yamamoto T. Direct Effect of Subthalamic Nucleus Stimulation on Levodopa-Induced Peak-Dose Dyskinesia in Patients with Parkinson’s Disease. Stereotact Funct Neurosurg. 2006;84(4):176-179. doi:10.1159/000094957 8. Teixeira AL, Maia DP, Cardoso F. UFMG Sydenham’s chorea rating scale (USCRS): reliability and consistency. Mov Disord. 2005;20(5):585-591. doi:10.1002/mds.20377 9. Tykocki T, Nauman P, Koziara H, Mandat T. Microlesion Effect as a Predictor of the Effectiveness of Subthalamic Deep Brain Stimulation for Parkinson’s Disease. Stereotact Funct Neurosurg. 2013. doi:10.1159/000342161 10. Oyama G, Maling N, Avila-Thompson A, et al. Rescue GPi-DBS for a Stroke-associated Hemiballism in a Patient with STN-DBS. Tremor Other Hyperkinet Mov (N Y). 2014;4. doi:10.7916/D8XP72WF 11. McLellan DL, Dean BC. Improved control of brittle Parkinsonism by separate administration of levodopa and benserazide. Br Med J (Clin Res Ed). 1982;284(6321):1001-1002. doi:10.1136/bmj.284.6321.1001 12. Martinez-Ramirez D, Giugni J, Vedam-Mai V, et al. The “brittle response” to Parkinson’s disease medications: Characterization and response to deep brain stimulation. PLoS One. 2014. doi:10.1371/journal.pone.0094856 13. Bostan AC, Strick PL. The basal ganglia and the cerebellum: Nodes in an integrated network. Nat Rev Neurosci. 2018. doi:10.1038/s41583-018-0002-7 14. Avecillas-Chasin JM, Honey CR. Modulation of Nigrofugal and Pallidofugal Pathways in Deep Brain Stimulation for Parkinson Disease. Neurosurgery. 2020. doi:10.1093/neuros/nyz544 15. Papa SM, Desimone R, Fiorani M, Oldfield EH. Internal globus pallidus discharge is nearly suppressed during levodopa- induced dyskinesias. Ann Neurol. 1999. doi:10.1002/1531-8249(199911)46:5<732::AID-ANA8>3.0.CO;2-Q 16. Suarez JI, Verhagen Merman L, Reich SG, Dougherty PM, Hallett M, Lenz FA. Pallidotomy for hemiballismus: Efficacy and characteristics of neuronal activity. Ann Neurol. 1997. doi:10.1002/ana.410420519 17. Bouthour W, Béreau M, Kibleur A, et al. Dyskinesia-inducing lead contacts optimize outcome of subthalamic stimulation in Parkinson’s disease. Mov Disord. 2019;34(11):1728-1734. doi:10.1002/mds.27853 18. Lanciego JL, Luquin N, Obeso JA. Functional neuroanatomy of the basal ganglia. Cold Spring Harb Perspect Med. 2012. doi:10.1101/cshperspect.a009621 19. Rodriguez-Rojas R, Carballo-Barreda M, Alvarez L, et al. Subthalamotomy for Parkinson’s disease: clinical outcome and topography of lesions. J Neurol Neurosurg Psychiatry. 2017. doi:10.1136/jnnp-2017-316241 20. Horn A, Li N, Dembek TA, et al. Lead-DBS v2: Towards a comprehensive pipeline for deep brain stimulation imaging. Neuroimage. 2019;184:293-316. doi:10.1016/j.neuroimage.2018.08.068
To cite this abstract in AMA style:
J. Avecillas Chasin, J. Jimenez-Shahed, J. Miravite, S. Bressman, B. Kopell. Deep brain stimulation of the pallidofugal pathways to rescue severe brittle dyskinesias after STN-DBS lead implantation [abstract]. Mov Disord. 2021; 36 (suppl 1). https://www.mdsabstracts.org/abstract/deep-brain-stimulation-of-the-pallidofugal-pathways-to-rescue-severe-brittle-dyskinesias-after-stn-dbs-lead-implantation/. Accessed March 27, 2026.« Back to MDS Virtual Congress 2021
MDS Abstracts - https://www.mdsabstracts.org/abstract/deep-brain-stimulation-of-the-pallidofugal-pathways-to-rescue-severe-brittle-dyskinesias-after-stn-dbs-lead-implantation/