Category: Rating Scales
Objective: Objective: The objective was to determine the association of the Fahn-Tolosa-Marin Clinical Rating Scale for Tremor (CRST) scores with the CRST global assessment.
Background: Background: The CRST is a commonly used three-part instrument to assess tremor severity in clinical trials.1–4 Part A is an assessment of tremor severity by body part. Part B assesses the performance of motor tasks such as writing or drawing. Part C evaluates functional disability secondary to tremor such as speaking, eating, and drinking. The CRST concludes with a global assessment of impairment completed by both the patient and examiner that is not incorporated into the total score. Given the use of the CRST in determining the efficacy of procedures for essential tremor, the correlation between CRST scores and global sense of impairment is worthy of investigation.
Method: Methods: This cross-sectional study includes patients who completed a CRST within the electronic health record of a tertiary health system from 2013 to 2023. The global assessment was rated on a 0 (no impairment) to 100% (most severe impairment) scale.
Results: Results: 138 patients were included (Table 1). Figure 1 depicts the relationship between the global assessments and total CRST scores. The total score was significantly associated with both the examiner-reported (Spearman’s correlation coefficient (ρ) 0.65 (95% confidence interval (CI) 0.54 – 0.73), p <0.001) and patient-reported global assessments (ρ 0.23 (95% CI 0.06 – 0.40, p = 0.01). Figure 2 demonstrates the relationships between the global ratings and CRST sub-scores. There was a significant association between the examiner-reported global rating and all three sub-scores (p < 0.001 for Parts A – C). There was not a significant association between Part A and the patient-reported global assessment (ρ 0.12 (95% CI -0.06 – 0.29, p = 0.17).
Conclusion: Conclusions: There is a clear discrepancy between patients and examiners in the relative strength of association between CRST scores and global assessment of impairment. Part A, a majority of the possible CRST point total, may have limited relevance to the patient’s impression of impairment. The impact of tremor is likely determined by functional detriments not readily measured with the CRST instrument. Specific aspects of a patient’s occupation, hobbies, or daily routine likely have an important influence on living with tremor and emphasize the value of patient-reported outcomes.
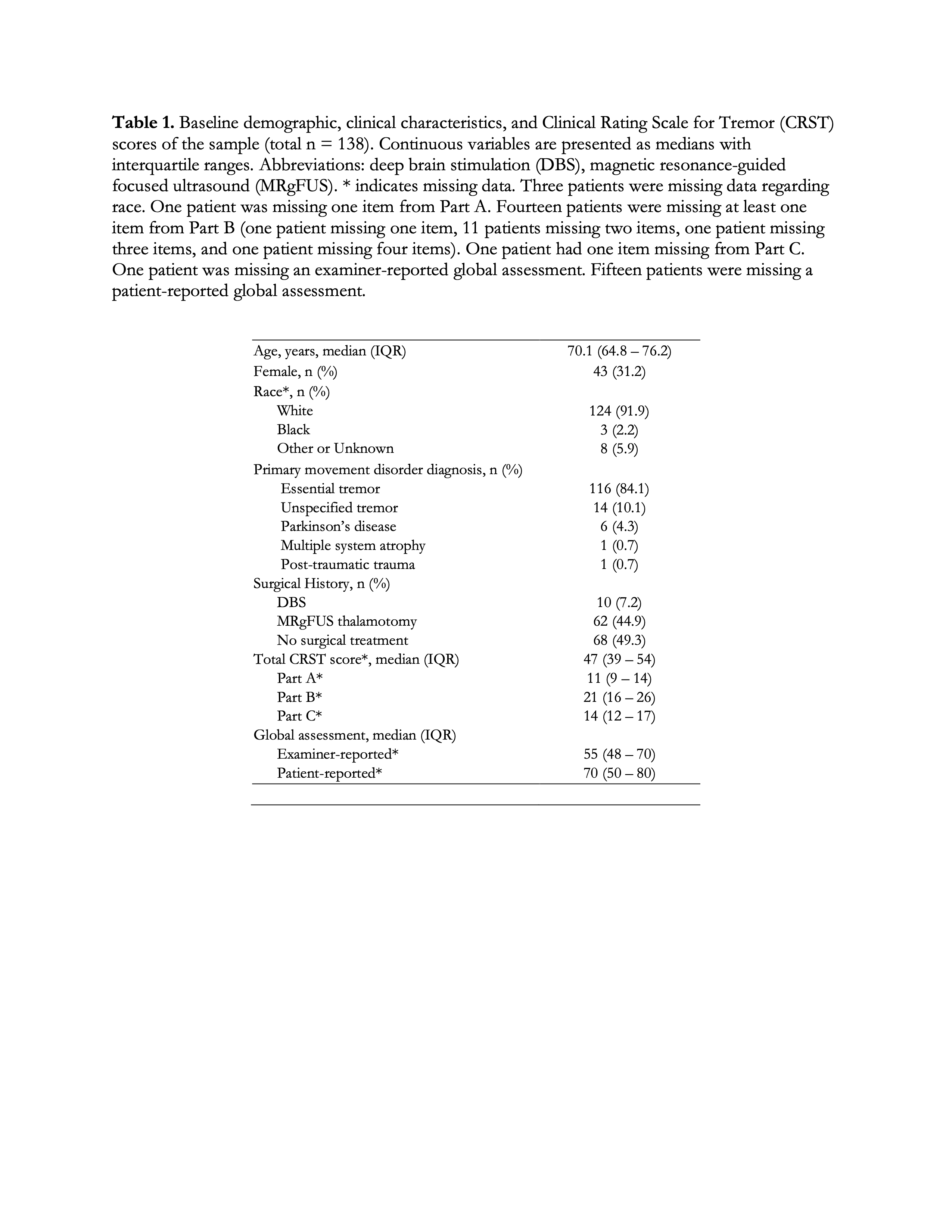
Table 1
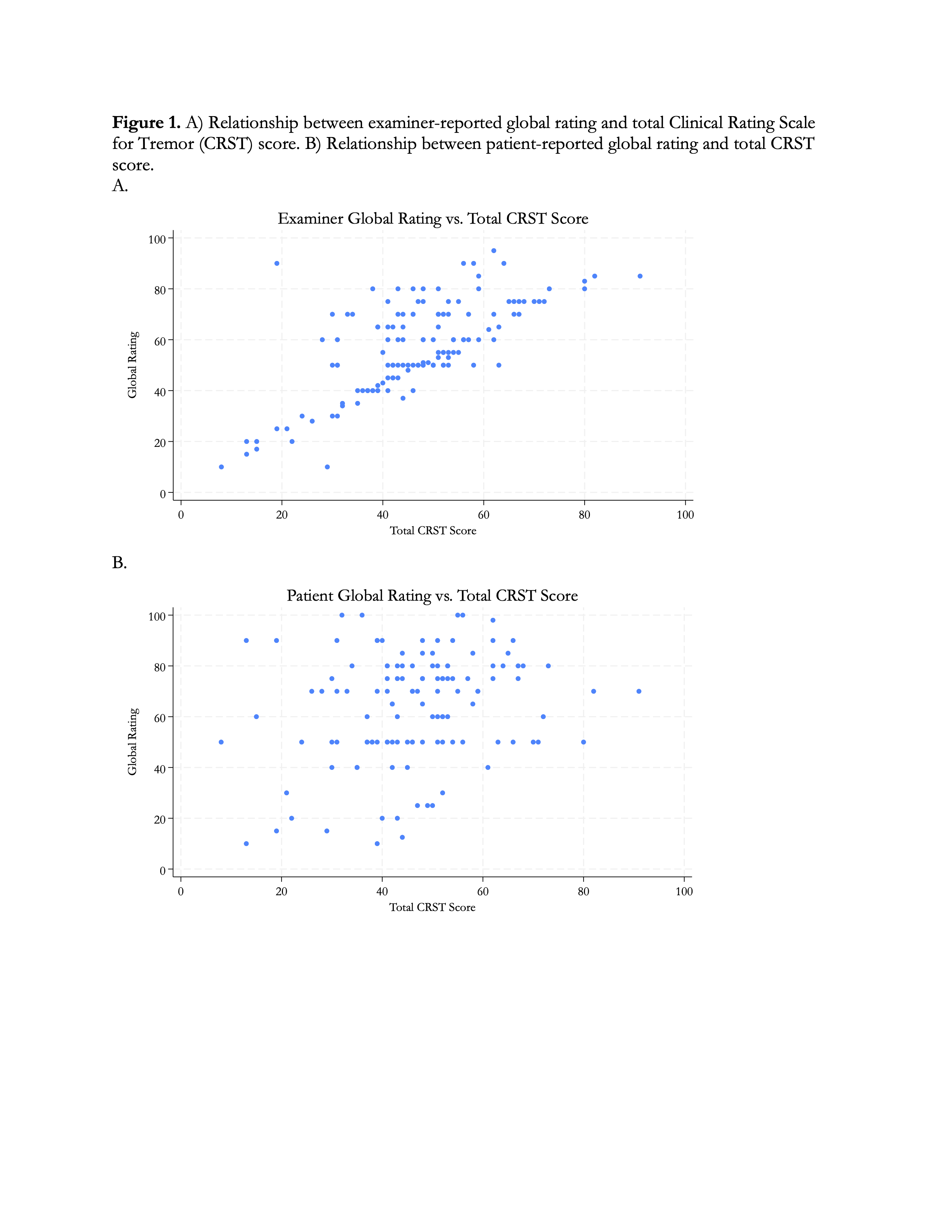
Figure 1
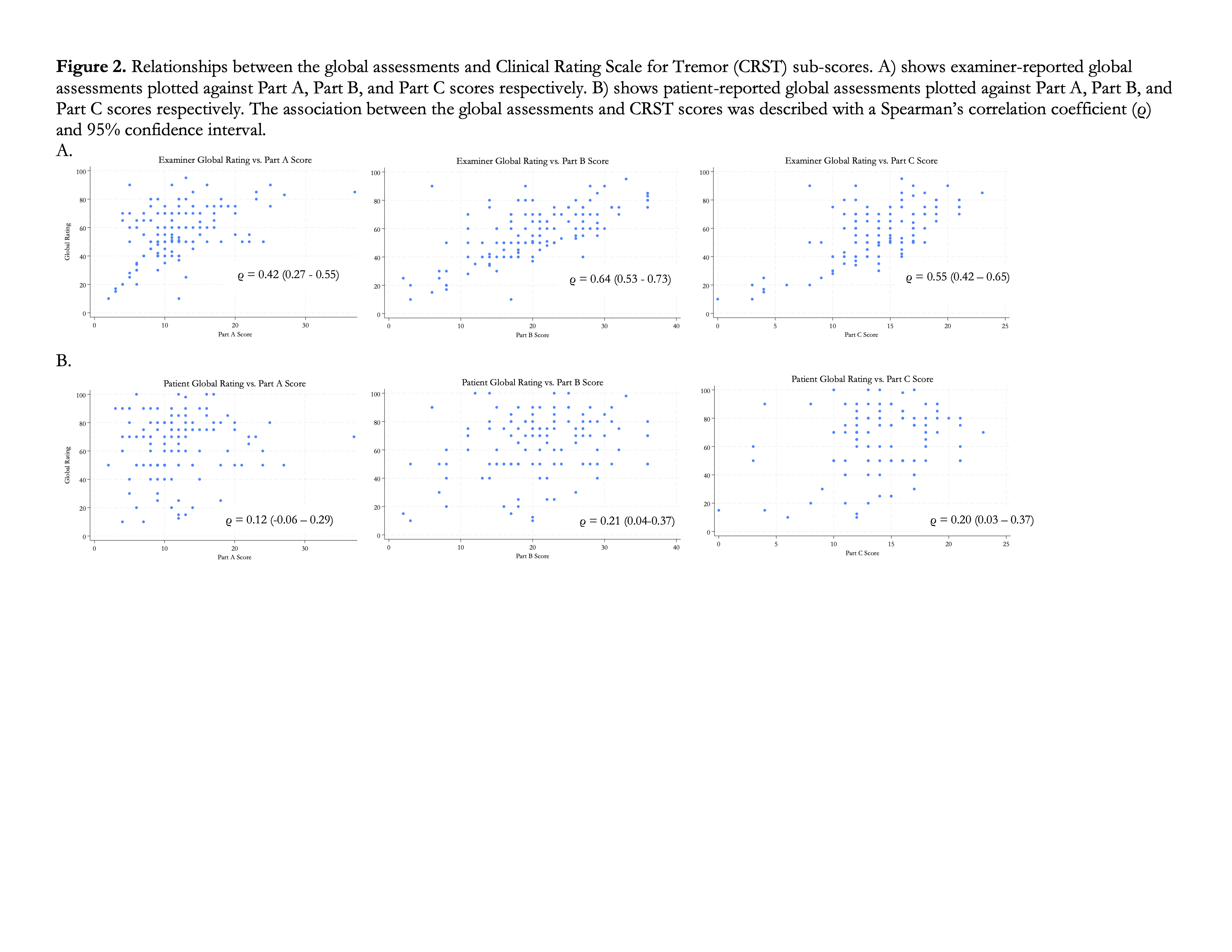
Figure 2
References: 1. Fahn S, Tolosa E, Marin C. Clinical Rating Scale for Tremor. 1988;2:271-280.
2. Elias WJ, Lipsman N, Ondo WG, et al. A Randomized Trial of Focused Ultrasound Thalamotomy for Essential Tremor. N Engl J Med. 2016;375(8):730-739. doi:10.1056/NEJMoa1600159
3. Elble RJ, Biondi DM, Ascher S, Wiegand F, Hulihan J. Carisbamate in essential tremor: brief report of a proof of concept study. Mov Disord. 2010;25(5):634-638. doi:10.1002/mds.22872
4. Zesiewicz TA, Sullivan KL, Hinson V, et al. Multisite, double-blind, randomized, controlled study of pregabalin for essential tremor. Mov Disord. 2013;28(2):249-250. doi:10.1002/mds.25264
To cite this abstract in AMA style:
S. Howard, S. Singh, D. Macaluso, J. Hsu, I. Cajigas, L. Qiu, C. Halpern, W. Aamodt, J. Farrar. Correlation of Clinical Rating Scale for Tremor with Global Assessment [abstract]. Mov Disord. 2024; 39 (suppl 1). https://www.mdsabstracts.org/abstract/correlation-of-clinical-rating-scale-for-tremor-with-global-assessment/. Accessed August 9, 2026.« Back to 2024 International Congress
MDS Abstracts - https://www.mdsabstracts.org/abstract/correlation-of-clinical-rating-scale-for-tremor-with-global-assessment/