Session Information
Date: Sunday, October 7, 2018
Session Title: Tremor
Session Time: 1:45pm-3:15pm
Location: Hall 3FG
Objective: To describe a case series of Holmes tremor (HT) from Movement Disorders Outpatient Clinic at the Clinical Hospital of State University of Campinas, from 2015-2017.
Background: HT is a rare symptomatic movement disorder, characterized by a combination of resting, postural, and action tremor. This tremor is also known as rubral, mesencephalic, or thalamic, but these terms are no longer used because typical cases have been described with lesions located in other areas. It is usually caused by lesions involving the brainstem, thalamus and cerebellum, mostly secondary to stroke, trauma or intracranial mass lesion. The pathophysiology of Holmes tremor is believed to result from a dysfunction of the dopaminergic system, in the nigrostriatal and cerebellothalamic pathways. It typically occurs with a delay, from 4 weeks to 2 years between the moment of lesion formation and the first occurrence of tremor, might be due to neuroplasticity.
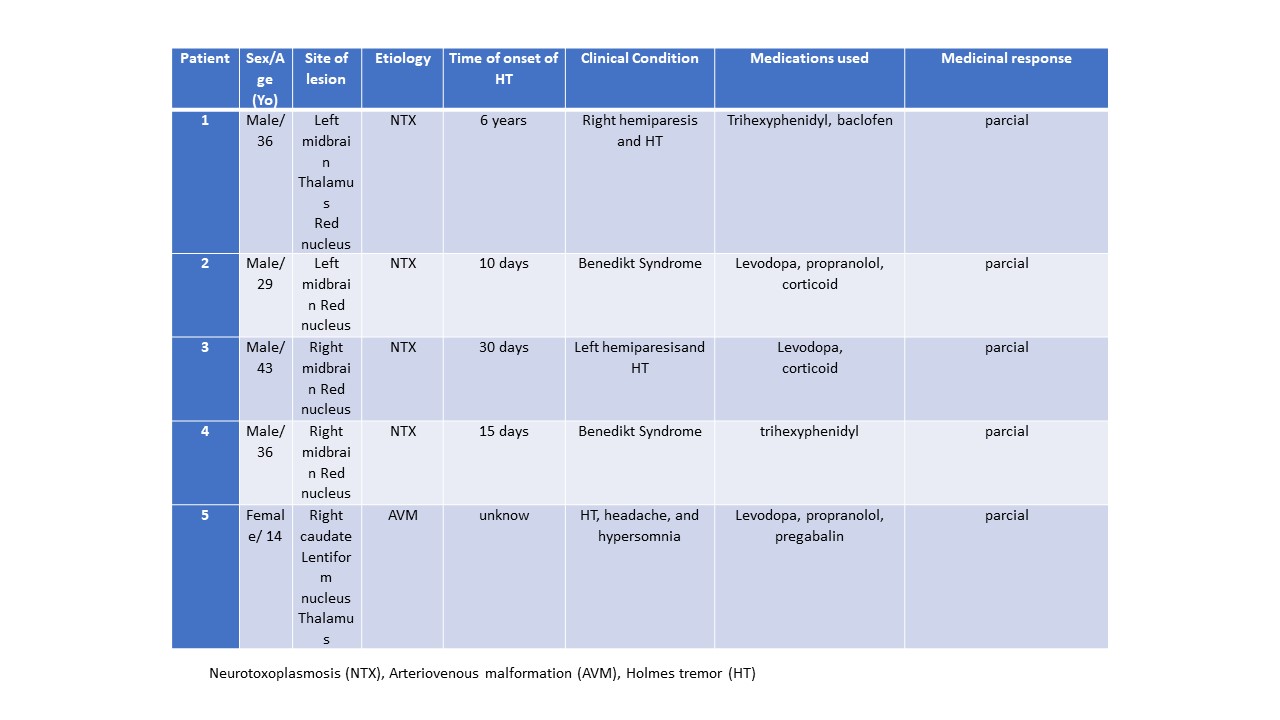
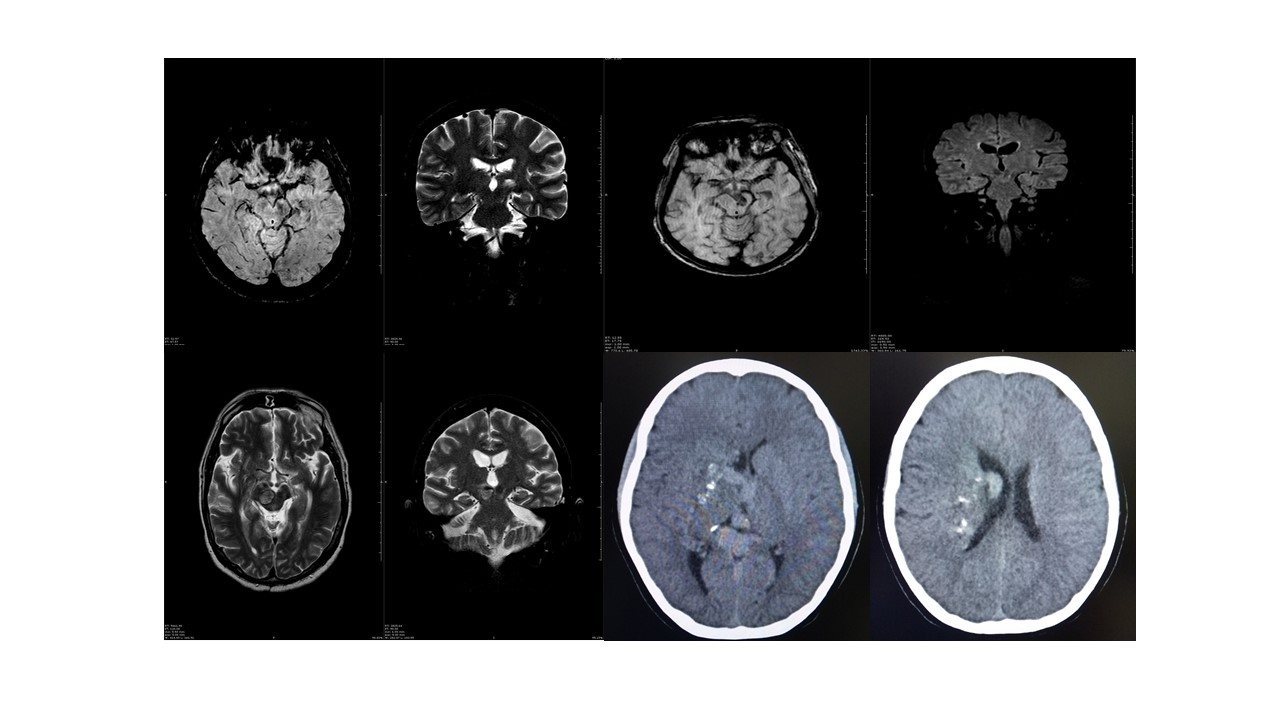
Methods: We evaluated 5 patients. Four cases were secondary to neurotoxoplasmosis (NTX) in patients with acquired immunodeficiency syndrome (AIDS), and another patient with HT secondary to arteriovenous malformation (AVM). All patients underwent neurological and cognitive evaluations, brain magnetic resonance imaging or cerebral angiography, which showed lesions in the mesencephalic tegmentum.
Results: Two of the 4 cases (29-43yo males) with HT secondary to NTX had Benedickt Syndrome, and the other 2 manifested hemiparesis due to contralateral midbrain lesion. The median latency from lesion to tremor onset was 2 weeks (range 10 days – 6 years). The fifth reported case (13yo female) manifested HT, headache, and hypersomnia as initial symptoms probably due to the location of AVM. Two cases of NTX were corticosteroid-responsive during a period. A variety of other drugs were used including levodopa, trihexyphenidyl, propranolol, pregabalin, and baclofen, all of them with poor response.
Conclusions: Pharmacological treatment is usually not very effective for HT, and surgical procedures (stereotactic thalamotomy or deep brain stimulation in ventralis intermedius nucleus of thalamus) are the gold-standard treatment to HT. Apart from that, the importance of this case series is the description of a rare tremor and brainstem syndrome as the clinical presentation of a very prevalent disease in the context of AIDS, such as NTX. Besides that, to highlight the complexity of its management.
References: Raina GB, Cersosimo MG, Folgar SS, Giugni JC, Calandra C, Paviolo JP, et al. Holmes tremor: clinical description, lesion localization, and treatment in a series of 29 cases. Neurology 2016;86:931–938. Lekoubou et al., Cerebral toxoplasmosis in Acquired Immunodeficiency Syndrome (AIDS) patients also provides unifying pathophysiologic hypotheses for Holmes tremor BMC Neurology 2010, 10:37.
To cite this abstract in AMA style:
F. de Moraes, F. de Paula, S. Filho, P. de Azevedo, L. Piovesana. Case series of Holmes tremor at the Clinical Hospital of State University of Campinas [abstract]. Mov Disord. 2018; 33 (suppl 2). https://www.mdsabstracts.org/abstract/case-series-of-holmes-tremor-at-the-clinical-hospital-of-state-university-of-campinas/. Accessed April 20, 2025.« Back to 2018 International Congress
MDS Abstracts - https://www.mdsabstracts.org/abstract/case-series-of-holmes-tremor-at-the-clinical-hospital-of-state-university-of-campinas/