Category: Choreas (Non-Huntington's Disease)
Objective: Given its rare incidence, there was a limited study reporting Fahr’s Disease (FD) presenting as chorea.
Background: FD is a rare condition characterized by intracranial calcifications in the basal ganglia with a prevalence rate of only 4,5 per 1.000 people.[1] Cognitive symptoms, psychiatric symptoms, and movement disorders may appear as clinical symptoms.[2,3]
Method: We present a case of A 58-year-old woman, with a history of diabetic mellitus, who complained of flowing, irregular, involuntary hyperkinetic movements involving the shoulder, the right arm, and leg from proximal to distal. Initially occurred on the right side of the body, and the movements worsened to the left side. It ceases during sleep and the phenomenology was consistent with chorea. The older sibling was experiencing similar complaints, but further examination was never conducted. Laboratory investigations revealed a normal glucose, calcium, and serum parathyroid level. Other potential organic etiologies were ruled out by normal laboratory parameters. Brain CT showed calcifications in the right caudate nucleus, bilateral lentiform nucleus, and bilateral cerebellum hemisphere.[Figure 1]
Results: Establishing the diagnosis of FD involves distinguishing it from Fahr’s syndrome.[4] The onset age of FD typically falls between 40 and 50, with adult patients primarily experiencing psychiatric or cognitive disorders, while older patients predominantly develop movement disorders.[1] A systematic review comprising 20 studies and 137 cases of FD revealed that chorea was reported in only 15% of cases, while parkinsonism was the most common manifestation of movement disorders. Basal ganglia calcification was a typical finding on brain CT scans, observed in all patients. Some cases also reported calcification in other areas such as the thalamus, dentate nucleus, and cortical regions. The study also demonstrates the correlation between the clinical manifestations and pathophysiology of FD with underlying genetics, including SLC20A2 associated with inorganic phosphate transporter defect, PDGFRB and PDGF B associated with blood-brain barrier regulation, and XPR1 associated with parathyroid hormone resistance.[5]
Conclusion: The symptoms that manifest in FD can vary depending on the onset and genetic etiology. Genetic testing is recommended in patients suspected of having FD to establish the underlying pathogenesis.
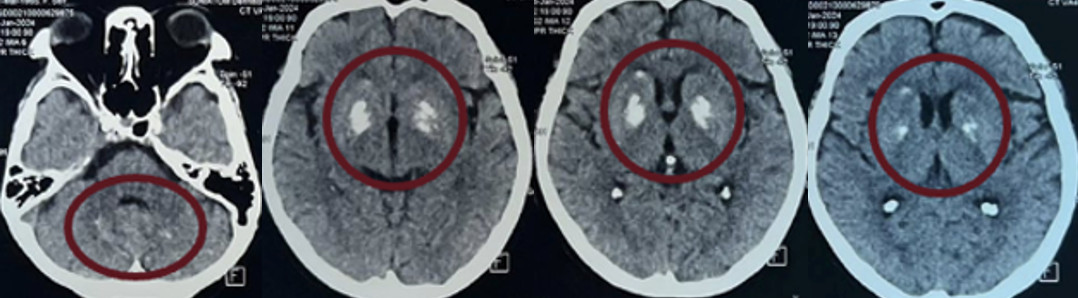
Figure 1. Brain CT showed calcifications
References: 1. Peters MEM, de Brouwer EJM, et al. Mechanisms of calcification in Fahr disease and exposure of potential therapeutic targets. Clinical Practice Month 2019 vol. 00 no. 00 1-9 doi:10.1212/CPJ.0000000000000782
2. Carecchio M, Barzhagi C, Varrasi C, Cantello L, Garavaglia B. Adult-Onset Focal Chorea in Fahr’s Disease Resulting From SLC20A2 Mutation: A Novel Phenotype. International Parkinson and Movement Disorder Society. 2014. doi:10.1002/mdc3.12114
3. Otu AA, Anikwe JC, Cocker D. Fahr’s disease: a rare neurological presentation in a tropical setting. Clinical Case Reports 2015; 3(10): 806–808. doi: 10.1002/ccr3.349
4. Ooi HW, Er C, Hussain I, Kuthiah N, Aravamudan VM. Bilateral Basal Ganglia Calcification: Fahr’s Disease. Cureus 11(6): e4797. 2019. DOI 10.7759/cureus.4797
5. Batla A, Tai XY, Schottlaender L, Erro R, Ballint B, Bhatia KP. Deconstructing Fahr’s disease/syndrome of brain calcification in the era of new genes. Elsevier. 2016
To cite this abstract in AMA style:
DA. Soraya, A. Tiksnadi, D. Tunjungsari. Fahr’s Disease Presenting as Chorea: A Rare Case Report [abstract]. Mov Disord. 2024; 39 (suppl 1). https://www.mdsabstracts.org/abstract/fahrs-disease-presenting-as-chorea-a-rare-case-report/. Accessed March 18, 2026.« Back to 2024 International Congress
MDS Abstracts - https://www.mdsabstracts.org/abstract/fahrs-disease-presenting-as-chorea-a-rare-case-report/