Objective: To describe a case of genetically proven neuroferritinopathy with isolated dystonic leg cramps and normal neuro-imaging.
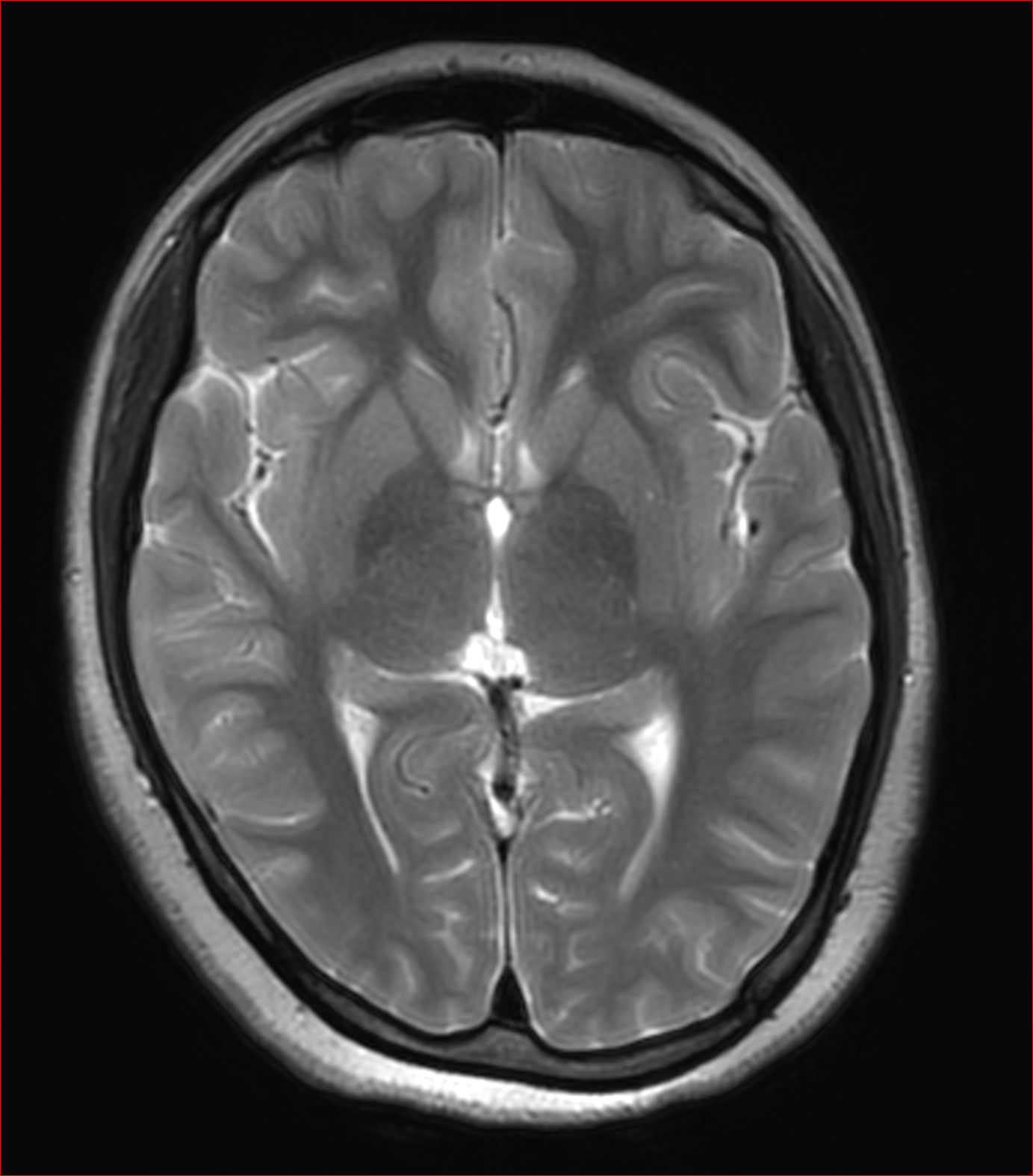
Background: Neuroferritinopathy(NF) is an autosomal dominant condition characterized by iron accumulation in the basal ganglia and low serum ferritin level1. This disorder is caused by mutations in the ferritin light chain (FTL) gene1. The initial and characteristic sign in MRI is a hypointense T2 signal and blooming on susceptibility weighted imaging(SWI) of basal ganglia2. Even though NF presents with complex movement disorder, our patient had isolated dystonic leg cramps and had normal neuroimaging.
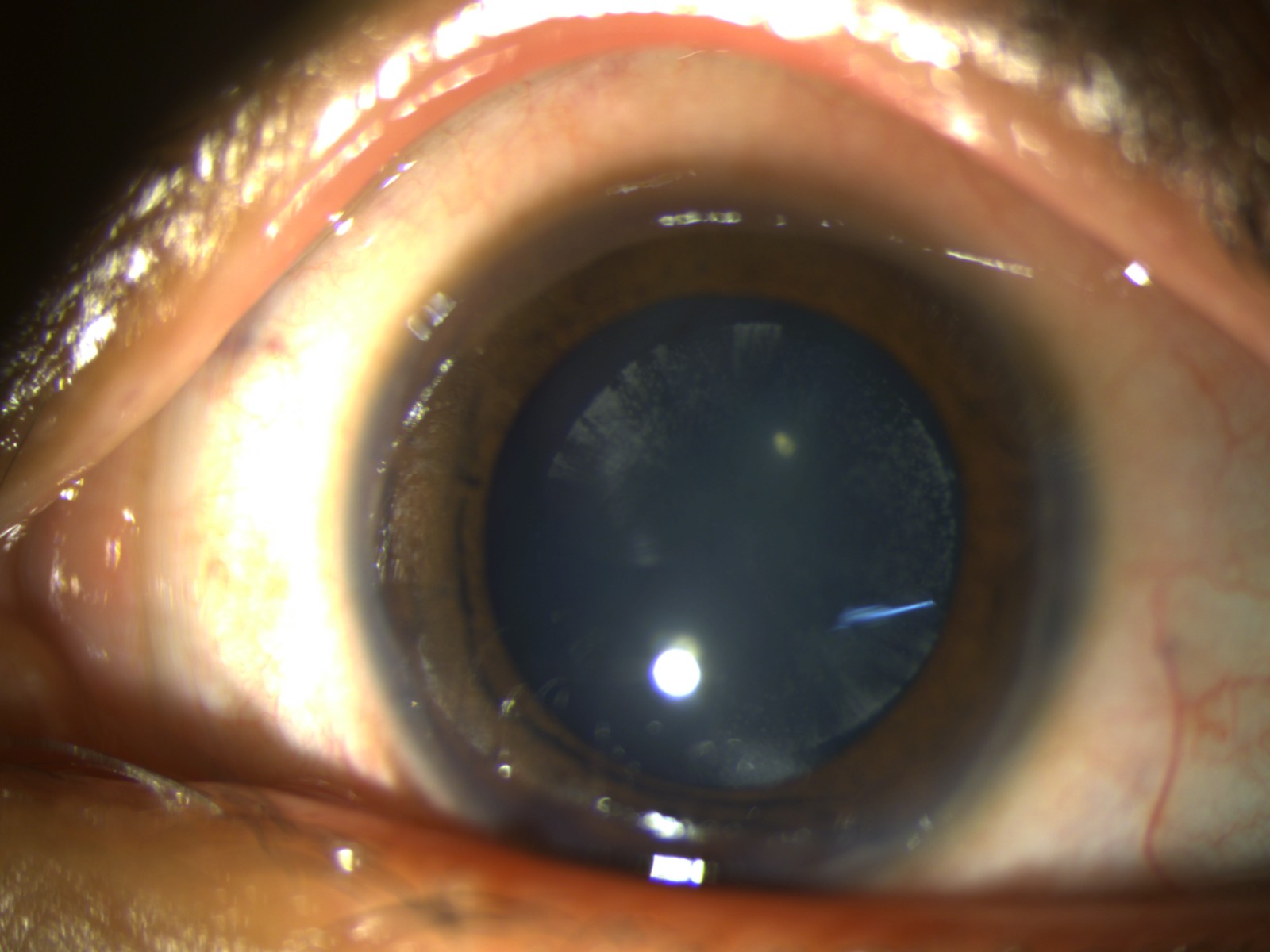
Method: 16-year-old girl, born from non-consanguineous marriage, presented with episodes of inward turning of the left ankle for 1 year and inward turning of the right ankle for 3 months, occurring at rest. These abnormal movements were periodic, involuntary, painless inversion of the right and left foot with toe extension lasting for 5- 8 minutes, without any diurnal variation. There was no history of cognitive impairment, pyramidal symptoms or other extrapyramidal symptoms. She has history of cataract in both eyes for which she was operated in one eye. Her family history was unremarkable. On examination, she had lamellar cataract in left eye and pseudophakia in right eye. Her general examination revealed absent antihelix bilaterally with right short fourth metatarsal and crossed-over toe.
Results: Considering a possibility of dopa responsive dystonia, she was started on levodopa-carbidopa with which she had satisfactory response. Biochemical testing for Wilson’s disease was normal, but serum ferritin level was low(<10 µg/L). Autoimmune serology, and peripheral smear for acanthocytes did not reveal any abnormality. MRI brain, including the SWI, was normal. Whole exome sequencing revealed FTL gene mutation at exon 3 [c.310G > T (p.Glu104Ter) variant]. This heterozygous nonsense variation in exon 3 resulted in a stop codon and premature truncation of the protein at codon 104. The p.Glu104ter variant was not reported in the 1000 genomes and gnomAD databases and was classified as pathogenic. Segregation analysis for parents was awaited at the time of presentation.
Conclusion: Our case exemplifies a rare phenomenon of normal neuroimaging in a genetically proven case of NF. Also, to the best of our knowledge, isolated dystonic leg cramps have not been described as the initial presentation in a case of NF.

References: 1. Lehn A, Boyle R, Brown H, Airey C, Mellick G. Neuroferritinopathy. Parkinsonism & Related Disorders. 2012 Sep 1;18(8):909-15.
2. Ohta E, Takiyama Y. MRI findings in neuroferritinopathy. Neurology research international. 2012 Oct;2012.
To cite this abstract in AMA style:
F. Mustafa, K. Sai Krishna, A. Das, A. Garg, A K. Srivastava. Case of neuroferritinopathy with isolated dystonic leg cramps and normal neuroimaging [abstract]. Mov Disord. 2023; 38 (suppl 1). https://www.mdsabstracts.org/abstract/case-of-neuroferritinopathy-with-isolated-dystonic-leg-cramps-and-normal-neuroimaging/. Accessed April 1, 2025.« Back to 2023 International Congress
MDS Abstracts - https://www.mdsabstracts.org/abstract/case-of-neuroferritinopathy-with-isolated-dystonic-leg-cramps-and-normal-neuroimaging/