Category: Surgical Therapy: Parkinson's Disease
Objective: To describe effects of thalamic deep brain stimulation (DBS) on severe dyskinesias induced by subthalamic nucleus (STN) DBS in a person with Parkinson’s disease (PD).
Background: STN DBS is an established treatment for PD with motor complications. Rarely, STN DBS induces bothersome dyskinesias that persist despite reduction in levodopa or activating dorsal contacts that stimulate pallidofugal fibers. In tremor-predominant PD, ViM DBS may be used for tremor control, but does not affect other Parkinsonian symptoms. A few reports suggest benefit from thalamotomy or ViM DBS on levodopa-induced dyskinesias [1,2,3]. To our knowledge, the effect of VIM DBS on STN DBS induced dyskinesias has not been described.
Method: A PD patient with bilateral STN and ViM DBS was assessed in clinic and by a blinded rater under multiple conditions using the Movement Disorders Society Unified Parkinson’s Disease Rating Scale, the Abnormal Involuntary Movements Scale, and the Patient Global Impression of Severity. The electrode locations were reviewed on post-operative imaging.
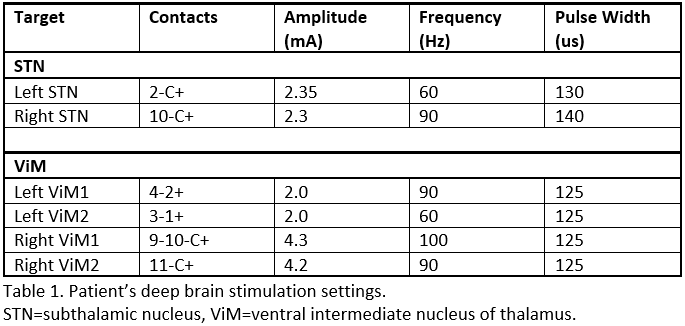
Results: A 59-year-old woman with 10 years of tremor-predominant, medication-refractory PD and levodopa intolerance underwent bilateral STN DBS in 2019. Prior to DBS, she had no dyskinesias. With activation of STN DBS, she developed severe cervical and truncal dyskinesias at low amplitudes. Dyskinesias did not abate over time despite usual anti-dyskinetic strategies. Tremors were uncontrolled due to inability to increase the amplitude over 1 mA without causing dyskinesias, so bilateral ViM DBS was implanted in 2021. Activation of ViM DBS controlled tremor and allowed STN amplitudes to be increased to improve bradykinesia, without inducing dyskinesias. When ViM DBS was turned off, severe dyskinesias immediately returned, and when turned back on, dyskinesias rapidly resolved. Results from blinded ratings will be presented. Active ViM contacts are more dorsal and anterior suggesting anti-dyskinetic effect may be due to spread of stimulation into ventral oralis anterior and posterior nuclei, the pallidal-receiving parts, of the thalamus [table1] [2].
Conclusion: In a patient with severe STN DBS induced dyskinesias, activation of thalamic DBS eliminated dyskinesias as well as tremor. Thalamic DBS can potentially be used as rescue therapy especially for tremor-predominant PD patients with STN DBS whose benefit is limited by dyskinesia.
References: 1. Narabayashi, H., Yokochi, F., & Nakajima, Y. (1984). Levodopa-induced dyskinesia and thalamotomy. Journal of neurology, neurosurgery, and psychiatry, 47(8), 831–839. https://doi.org/10.1136/jnnp.47.8.831
2. Caparros-Lefebvre, D., Blond, S., Vermersch, P., Pécheux, N., Guieu, J. D., & Petit, H. (1993). Chronic thalamic stimulation improves tremor and levodopa induced dyskinesias in Parkinson’s disease. Journal of neurology, neurosurgery, and psychiatry, 56(3), 268–273. https://doi.org/10.1136/jnnp.56.3.268
3. Caparros-Lefebvre, D., Blond, S., Feltin, M. P., Pollak, P., & Benabid, A. L. (1999). Improvement of levodopa induced dyskinesias by thalamic deep brain stimulation is related to slight variation in electrode placement: possible involvement of the centre median and parafascicularis complex. Journal of neurology, neurosurgery, and psychiatry, 67(3), 308–314. https://doi.org/10.1136/jnnp.67.3.308
To cite this abstract in AMA style:
D. Shah-Zamora, J. Karl, L. Verhagen. Elimination of STN stimulation-induced dyskinesias with ViM DBS [abstract]. Mov Disord. 2022; 37 (suppl 2). https://www.mdsabstracts.org/abstract/elimination-of-stn-stimulation-induced-dyskinesias-with-vim-dbs/. Accessed April 2, 2025.« Back to 2022 International Congress
MDS Abstracts - https://www.mdsabstracts.org/abstract/elimination-of-stn-stimulation-induced-dyskinesias-with-vim-dbs/