Category: Dystonia: Clinical Trials and Therapy
Objective: To investigate the course of the maxillary artery (MA) in relation to the lateral pterygoid muscle (LPM) in the Turkish population and to help to standardize the approach for botulinum neurotoxin (BoNT) injections of LPM in patients with oromandibular dystonia (OMD).
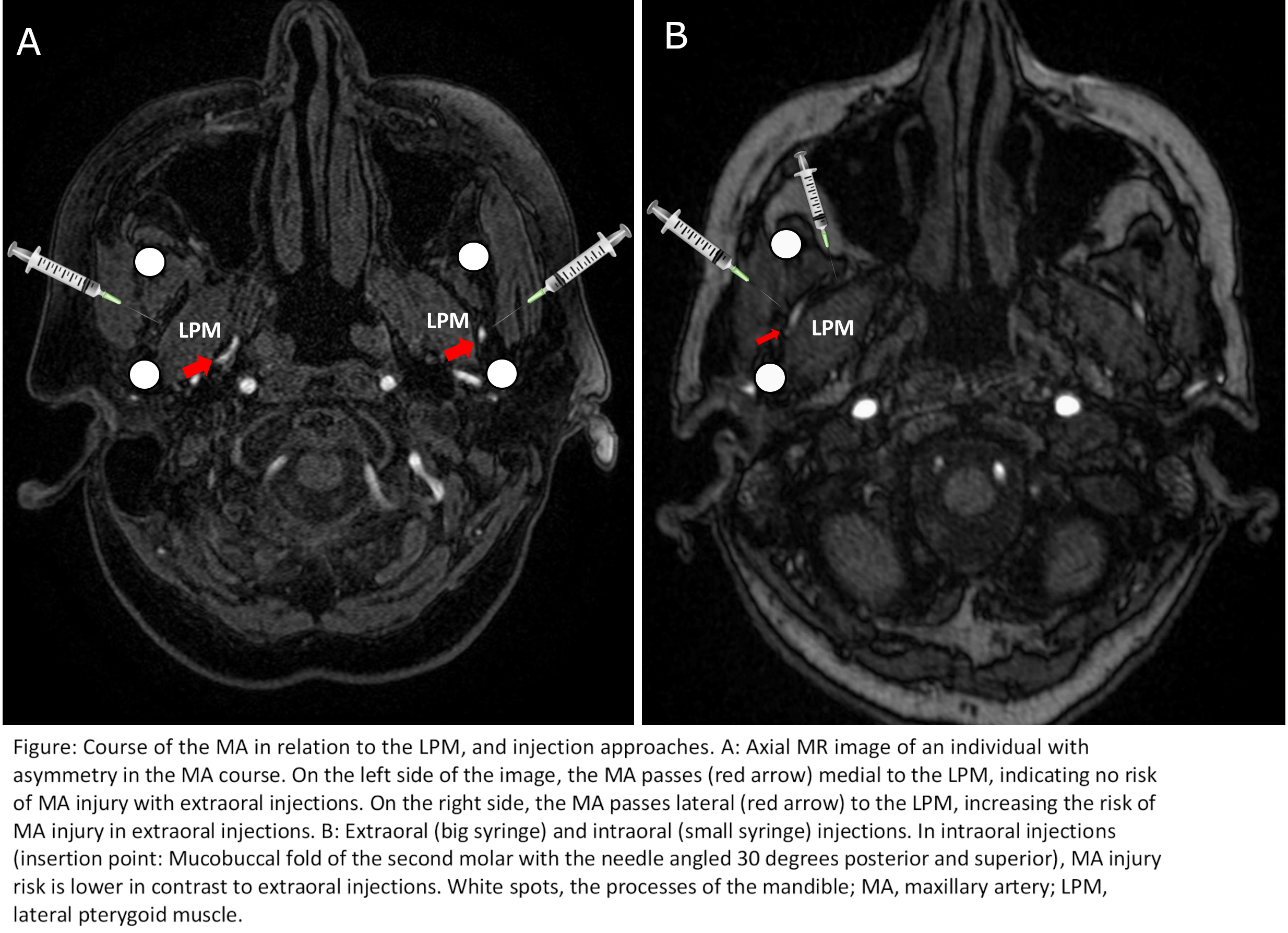
Background: Studies showed that the course of the MA varies considerably with respect to its proximity with the LPM [1], which has practical implications such as choosing between extraoral (preauricular transcutaneous) or intraoral approaches for BoNT injections in patients with OMD. In 93% of the Japanese population, MA runs lateral to the LPM (closer to the skin), whereas studies from Western societies reported a rate of around 62% [1]. These values indicate a high risk for MA injury in extraoral injections that may result in pain and hematoma [2] and thus, necessitate an intraoral approach (Figure). However, this critical anatomical variation is still unrecognized by most clinicians performing BoNT injections.
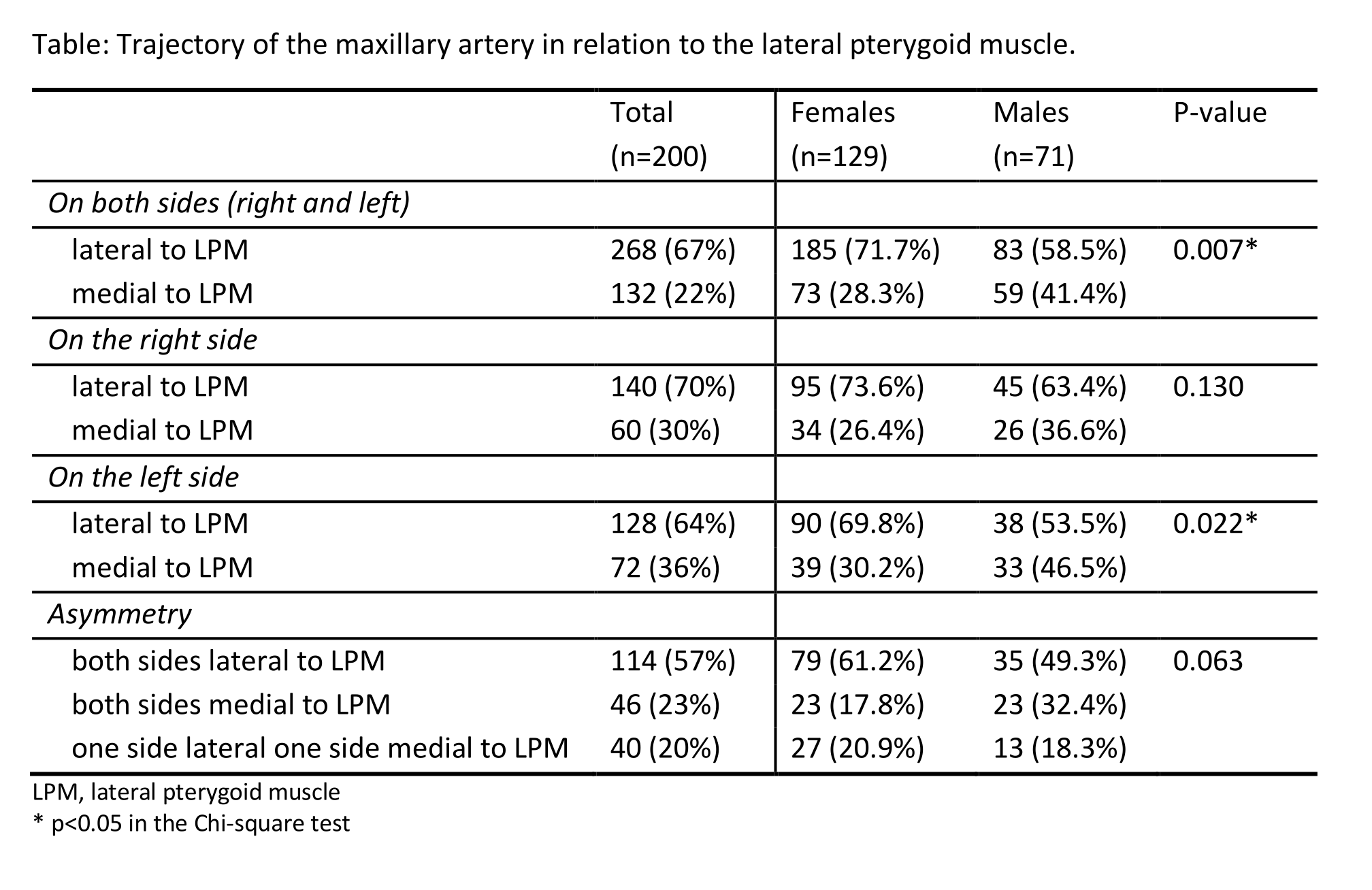
Method: Magnetic resonance angiography (MRA) images of 200 individuals without a history of facial trauma or movement disorders were evaluated by two neuroradiology experts. The course of the MA with respect to the LPM was assessed on both sides. Prevalence of MA running lateral to the LPM, gender-related differences, and asymmetry in the course of the MA were reported.
Results: A summary of the results is given in the Table. The participants had a mean age of 56.4 (±18.8) years, and 142 (64%) were female. The MA was passing laterally to the LPM in 67% of the evaluated sides in MRA. A significantly more frequent lateral course in females and an asymmetry between the right and left sides were detected in 20% of all assessments.
Conclusion: Similar to the previously reported rates of the caucasian population, the MA passes lateral to the LPM in around 2/3 of the Turkish participants. According to our findings, in patients with OMD needing BoNT injections to the LPM, an intraoral approach is safer to avoid MA injury.
References: 1. Maeda S, Aizawa Y, Kumaki K, Kageyama I. Variations in the course of the maxillary artery in Japanese adults. Anat Sci Int. 2012; 87(4): 187–194. 2. Yoshida K. Botulinum neurotoxin injection for the treatment of recurrent temporomandibular joint dislocation with and without neurogenic muscular hyperactivity. Toxins (Basel) 2018 Apr 25;10(5):174.
To cite this abstract in AMA style:
S. Unal, T. Karaarslan-Turk, C. Akbostanci, E. Peker, R. Yilmaz. Approaching the lateral pterygoid muscle in botulinum toxin injections. How to avoid the maxillary artery [abstract]. Mov Disord. 2021; 36 (suppl 1). https://www.mdsabstracts.org/abstract/approaching-the-lateral-pterygoid-muscle-in-botulinum-toxin-injections-how-to-avoid-the-maxillary-artery/. Accessed May 7, 2026.« Back to MDS Virtual Congress 2021
MDS Abstracts - https://www.mdsabstracts.org/abstract/approaching-the-lateral-pterygoid-muscle-in-botulinum-toxin-injections-how-to-avoid-the-maxillary-artery/