Category: Parkinson's Disease: Neuroimaging
Objective: The purpose of this study was to examine quantitative susceptibility mapping (QSM) changes in PD and multiple system atrophy with predominant parkinsonism (MSA-P) and progressive supranuclear palsy (PSP), and to clarify the differences.
Background: There have been already reports of using QSM to distinguish it from Parkinson’s disease (PD) and other atypical parkinsonism. However, it is not enough.
Method: This study was conducted retrospectively. Inclusion criteria were as follows: patients with PD, MSA-P and PSP who matched the clinical diagnosis criteria and underwent QSM imaging at our institution between November 2016 and June 2019. The subjects were 104 patients with PD (mean 68.5 years), 16 patients with PSP (mean 72.4 years), and 9 patients with MSA-P (mean 64.0 years).The multiple dipole-inversion combination with k-space segmentation method was used to create QSM images. We set substantia nigra(SN), red nucleus(RN), subthalamic nucleus(STN) globus pallidus(GP) and putamen(Put) as regions of interest, and examined the differences for each disease using the susceptibility value(SV) as an evaluation value.
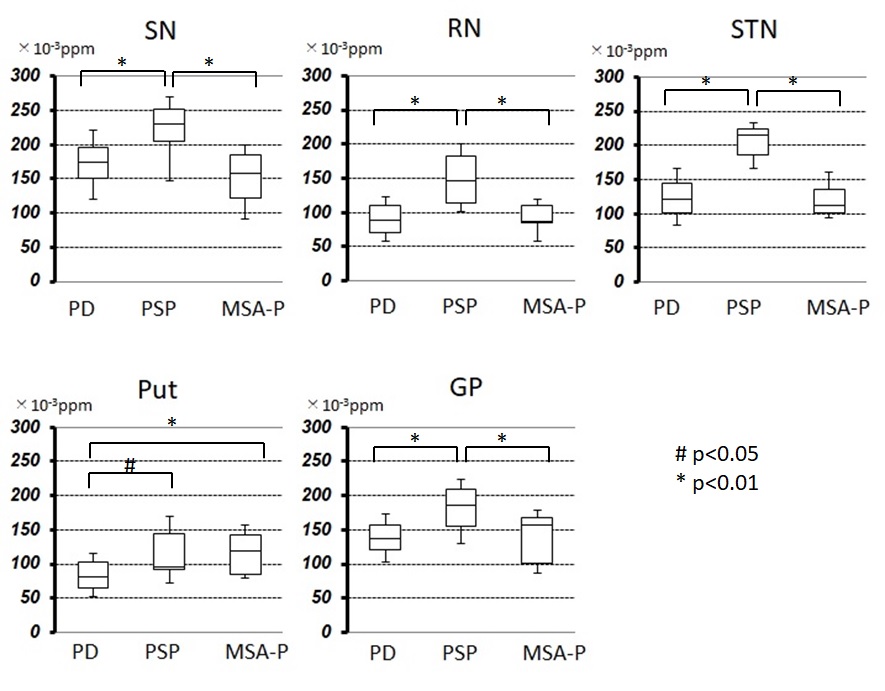
Results: The SV of Put in MSA-P and PSP was significant higher than that of PD(0.114, 0.113 vs 0.083, ANOVA p<0.01, Bonferroni both p<0.01). The SV of SN, RN, STN and GP in PSP was significant higher than that of PD and MSA-P(ANOVA p<0.01, SN;0.223 vs 0.173, 0.150, both p<0.01 RN;0.151 vs 0.089, 0.090, both p<0.01, STN; 0.206 vs 0.124, 0.121, both p<0.01, GP; 0.180 vs 0.142, 0.143, p<0.01, 0.05, respectively)(figure). The area under the ROC curve (AUC) for the SV of STN between PD and PSP was 0.953. AUC for the SV of RN between PD and PSP was 0.867. In addition, we have created an index that adds 3, 2, 1, and 1 points to those whose susceptibility value exceeds the threshold of 0.180 / 0.200 / 0.120 / 0.165 ppm in STN, SN, RN, and GP, respectively. This index was defined as PSP when the score was 5 or more. As a result, in distinguishing PSP from PD, sensitivity was 97.1% and specificity was 87.5%.
Conclusion: QSM may help distinguish PD, PSP, and MSA-P. AUC for the SV of STN between PD and PSP was 0.953 and the sensitivity and specificity of the diagnostic index was 97.1% and 87.5%, which suggested that QSM is especially usefull for distinguishing between PD and PSP.
References: Sjöström H, Granberg T, Westman E, Svenningsson P. Quantitative susceptibility mapping differentiates between parkinsonian disorders. Park Relat Disord. 2017;44:51–7. Takahashi H, Watanabe Y, Tanaka H, Mihara M, Mochizuki H, Takahashi K, et al. Comprehensive MRI quantification of the substantia nigra pars compacta in Parkinson’s disease. Eur J Radiol. 2018;109(June):48–56.
To cite this abstract in AMA style:
K. Matsuura, Y. Ii, M. Maeda, K. Tabei, M. Umino, H. Tomimoto, A. Shindo. Quantitative Susceptibility Mapping may help distinguish patients with Parkinson’s disease, progressive supranuclear palsy and multiple system atrophy with predominant parkinsonism [abstract]. Mov Disord. 2020; 35 (suppl 1). https://www.mdsabstracts.org/abstract/quantitative-susceptibility-mapping-may-help-distinguish-patients-with-parkinsons-disease-progressive-supranuclear-palsy-and-multiple-system-atrophy-with-predominant-parkinsonism/. Accessed July 4, 2026.« Back to MDS Virtual Congress 2020
MDS Abstracts - https://www.mdsabstracts.org/abstract/quantitative-susceptibility-mapping-may-help-distinguish-patients-with-parkinsons-disease-progressive-supranuclear-palsy-and-multiple-system-atrophy-with-predominant-parkinsonism/