Category: Dystonia: Pathophysiology, Imaging
Objective: To test the hypothesis that there is shared regional or global functional connectivity dysfunction in a large cohort with isolated focal dystonia affecting different body regions compared to control participants.
Background: Substantial evidence links basal ganglia dysfunction with focal dystonia, but recent neuroimaging studies implicate pathophysiologic contributions from other brain regions or related networks including cerebellum, sensorimotor cortical areas, brainstem and thalamus. Some of the purported network abnormalities may reflect inconsistent methods to address motion-related confounds in fMRI studies.
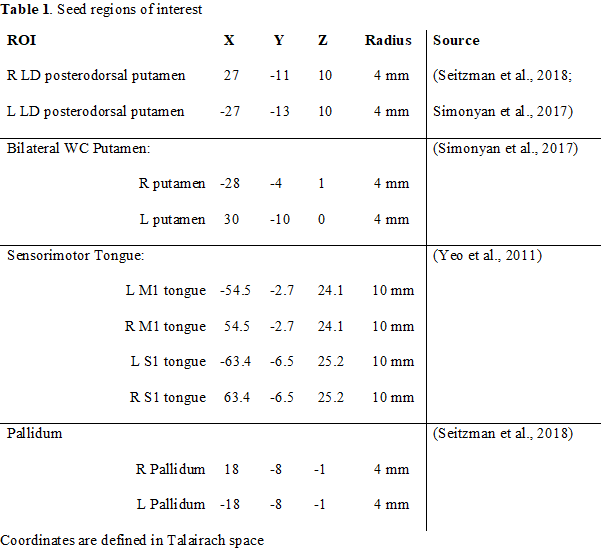
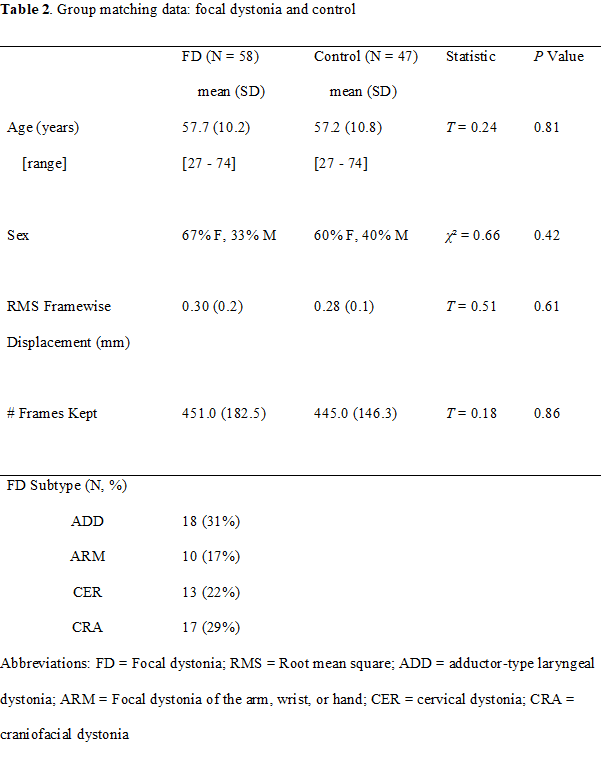
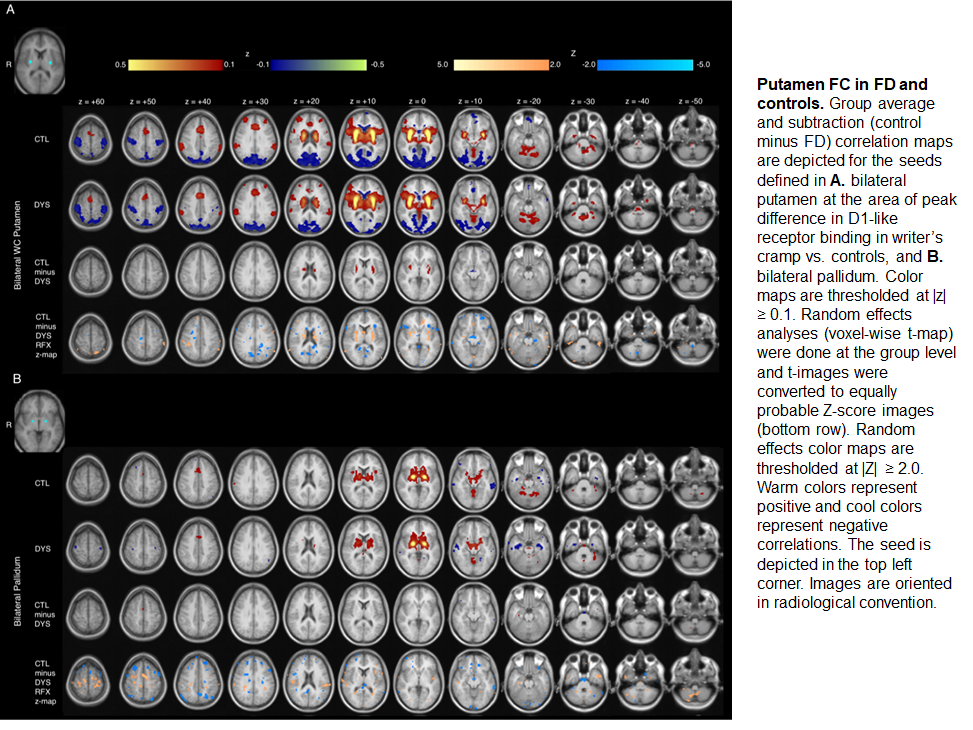
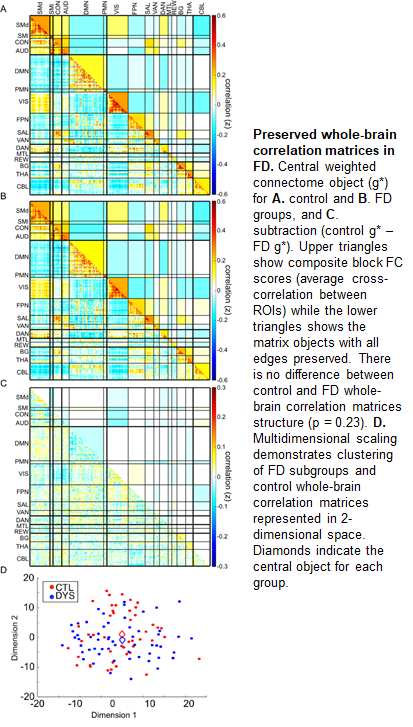
Method: We obtained resting-state MRI scans (3-4 scans, 7.3 minute runs) with eyes closed in participants with focal dystonia (cranial [17], cervical [13], laryngeal [18], limb [10]) and age- and sex-matched controls. Rigorous preprocessing [1-4] for all analyses was performed to minimize effect of head motion during scan acquisition (dystonia N=58, control N=47 analyzed). We assessed regional functional connectivity by computing a seed-correlation map between putamen, pallidum, and sensorimotor cortex and all brain voxels. Significant group differences were assessed on a cluster-wise basis. In a separate analysis, we applied 300 seed regions across the cortex, cerebellum, basal ganglia and thalamus to comprehensively sample the whole brain. Participant whole-brain correlation matrices were obtained by computing the correlation between seed average time courses for each seed pair. Group-level whole-brain differences were assessed using weighted object-oriented data analysis.
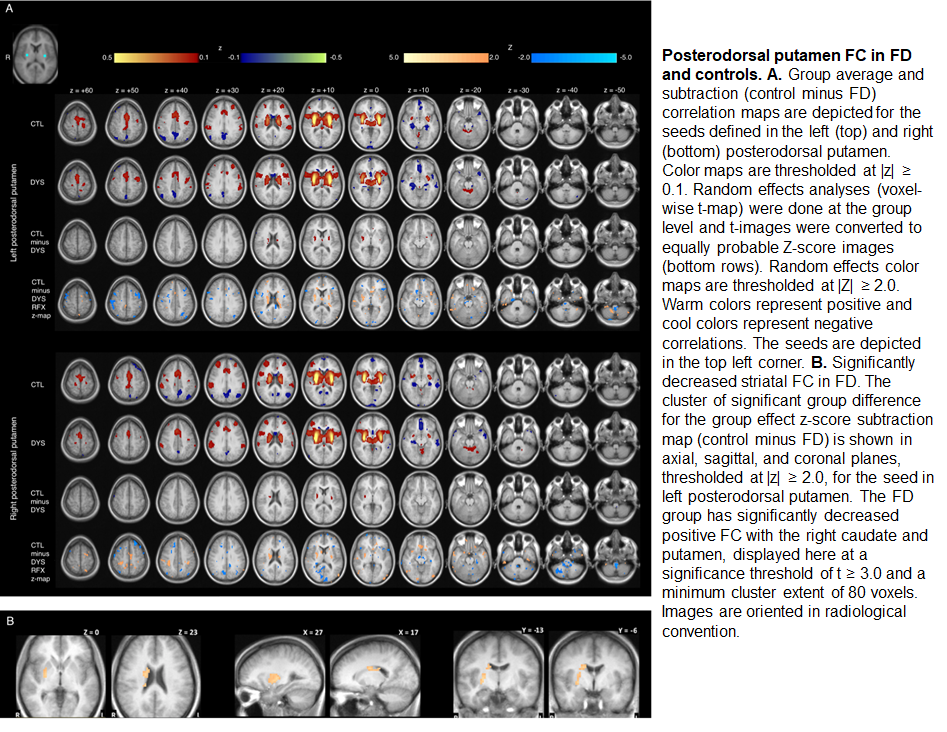
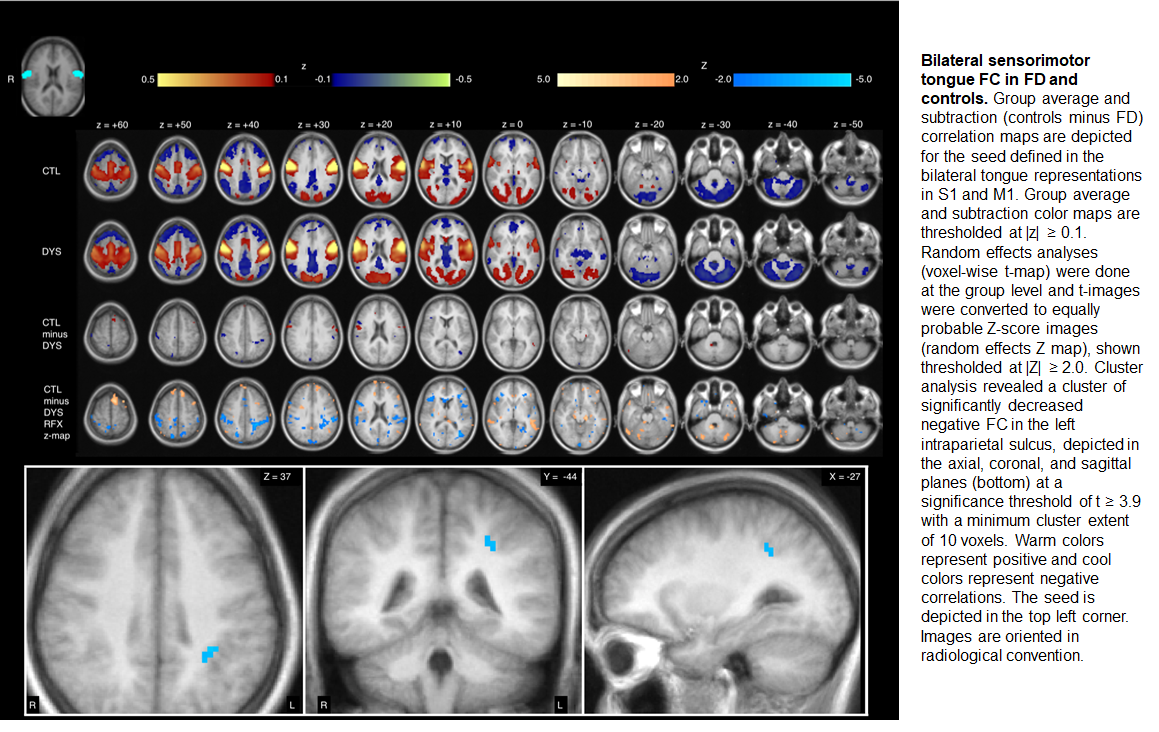
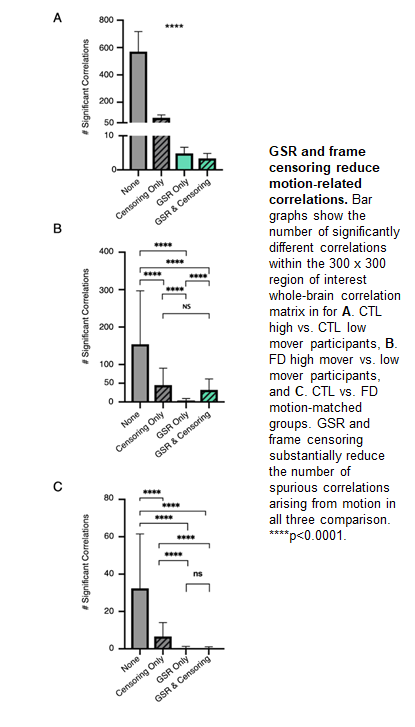
Results: Participants with focal dystonia had decreased functional connectivity at the regional level, within the striatum and between lateral primary sensorimotor cortex and ventral intraparietal area, whereas whole-brain correlation matrices do not differ between focal dystonia and control groups. Rigorous quality control measures eliminated spurious large-scale functional connectivity differences between groups.
Conclusion: Regional functional connectivity differences, not global network level dysfunction, contributes to common pathophysiological mechanisms in isolated focal dystonia. Rigorous quality control eliminated significant spurious large-scale network differences between focal dystonia and control participants. Data submitted as abstract, Samuel Belzberg 6th International Dystonia Symposium, Dublin Ireland, June 2020.
References: 1. Power JD, Barnes KA, Snyder AZ, Schlaggar BL, Petersen SE. Spurious but systematic correlations in functional connectivity MRI networks arise from subject motion. Neuroimage 2012;59:2142-2154. 2. Power JD, Mitra A, Laumann TO, Snyder AZ, Schlaggar BL, Petersen SE. Methods to detect, characterize, and remove motion artifact in resting state fMRI. Neuroimage 2014;84:320-341. 3. Li Z, Prudente CN, Stilla R, Sathian K, Jinnah HA, Hu X. Alterations of resting-state fMRI measurements in individuals with cervical dystonia. Hum Brain Mapp 2017;38:4098-4108. 4. Ciric R, Wolf DH, Power JD, et al. Benchmarking of participant-level confound regression strategies for the control of motion artifact in studies of functional connectivity. Neuroimage 2017;154:174-187.
To cite this abstract in AMA style:
S. Norris, A. Morris, M. Campbell, M. Karimi, A. Babatunde, R. Paniello, A. Snyder, J. Mink, J. Perlmutter. Regional, Not Global, Functional Connectivity Contributes to Isolated Focal Dystonia [abstract]. Mov Disord. 2020; 35 (suppl 1). https://www.mdsabstracts.org/abstract/regional-not-global-functional-connectivity-contributes-to-isolated-focal-dystonia/. Accessed March 13, 2026.« Back to MDS Virtual Congress 2020
MDS Abstracts - https://www.mdsabstracts.org/abstract/regional-not-global-functional-connectivity-contributes-to-isolated-focal-dystonia/