Session Information
Date: Tuesday, September 24, 2019
Session Title: Tics/Tourette
Session Time: 1:45pm-3:15pm
Location: Les Muses Terrace, Level 3
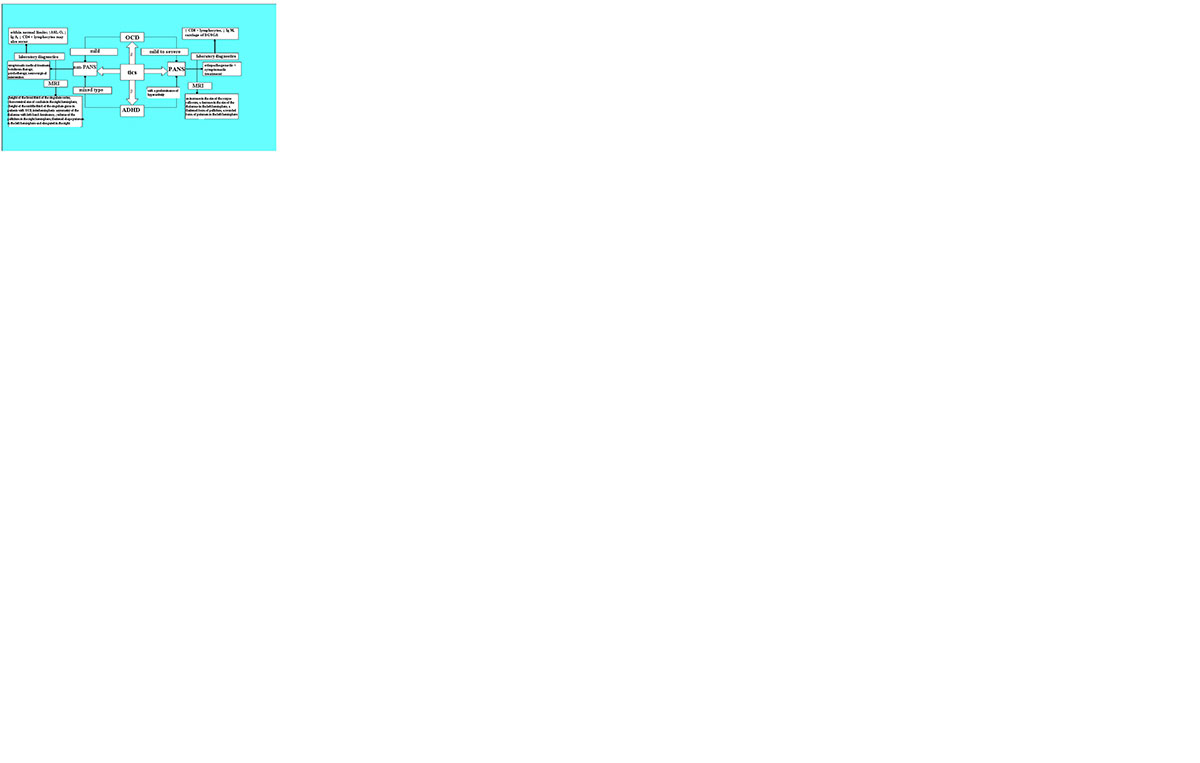
Objective: Develop an algorithm for diagnosis and differentiated approach to the management of patients with tics
Background: The prevalence of tics reaches 20%; often accompanied by obsessive-compulsive syndrome (OCD) and attention deficit hyperactivity disorder (ADHD).High prevalence, etiological and clinical heterogeneity, morphofunctional changes determine the need for further analysis
Method: The main group consisted of 111 patients. Two control groups consisted of 56 people. The patients were divided into 2 groups: “PANS-pediatric-onset neuropsychiatric syndrome” – “pediatric acute neuropsychiatric syndrome” and “non-PANS”.Research methods: 1)neurological examination; 2)laboratory clinical and immunological studies; 3)MRI of the brain with morphometry of the basal ganglia, thalamus, corpus callosum, cingulate gyrus.
Results: Patients with Tourette syndrome (TS) prevailed (33%). OCD was found in 53.2% tics with varying severity. The direct dependence of the severity of motor and vocal tics on the severity of OCD and ADHD (r = 0.54, p≤0.01) was determined. Tics were associated with ADHD with the prevalence of hyperactivity in 81% of cases.Clinical MRI-morphometric correlation was revealed: the dependence of motor and vocal tics on the heights of the middle and posterior third of the cingulate gyrus; increased frontal lobe in ADHD; increased dimensions of the cingulate gyrus and corpus callosum with OCD, modified forms of the puamen and the caudate nucleus, a smaller volume of the globus pallidum, inter-hemispheric asymmetry of the thalamus in patients with tics (p <0.05).PANS-syndrome was 2.5 times more common in males. The presence of a chronic focus of infection was not a predictor of the development of the syndrome. The PANS group was characterized by TS (39%), mild to severe OCD, ADHD with a predominance of hyperactivity, specific MRI-signs, clinical correlation with JgM, CD8 + lymphocytes and carriage β-hemolytic streptococcus group A (BGSGA)
Conclusion: Tic is the cause of pancerebral dysfunction, as a result of which they have a complex psychomotor “nature.” Impaired B-lymphocyte differentiation, lack of humoral response, special antigens that can cause an inadequate immune response, accompanied by a powerful release of cytokines, can be the basis for the launch of autoimmune disorders with neuronal tissue damage and as a result of the development of tic hyperkinesis
To cite this abstract in AMA style:
S. Munasipova, Z. Zalyalova. Algorithm of a differentiated approach to the management of patients with tic hyperkinesis [abstract]. Mov Disord. 2019; 34 (suppl 2). https://www.mdsabstracts.org/abstract/algorithm-of-a-differentiated-approach-to-the-management-of-patients-with-tic-hyperkinesis/. Accessed June 20, 2026.« Back to 2019 International Congress
MDS Abstracts - https://www.mdsabstracts.org/abstract/algorithm-of-a-differentiated-approach-to-the-management-of-patients-with-tic-hyperkinesis/