Session Information
Date: Tuesday, September 24, 2019
Session Title: Parkinsonisms and Parkinson-Plus
Session Time: 1:45pm-3:15pm
Location: Agora 3 West, Level 3
Objective: Objective: We aimed to correlate hand deformities in patients with Parkinson´s disease (PD) with demographics, motor status and other parkinsonian postural abnormalities in order to gain insights into contributing causes of such deformities and address whether these hand deformities are predictors of advanced PD, dyskinesia, worse motor and cognitive status.
Background: Background: Hand deformities have been recognized since the XIX century as part of the postural abnormalities observed in Parkinson´s disease (PD).
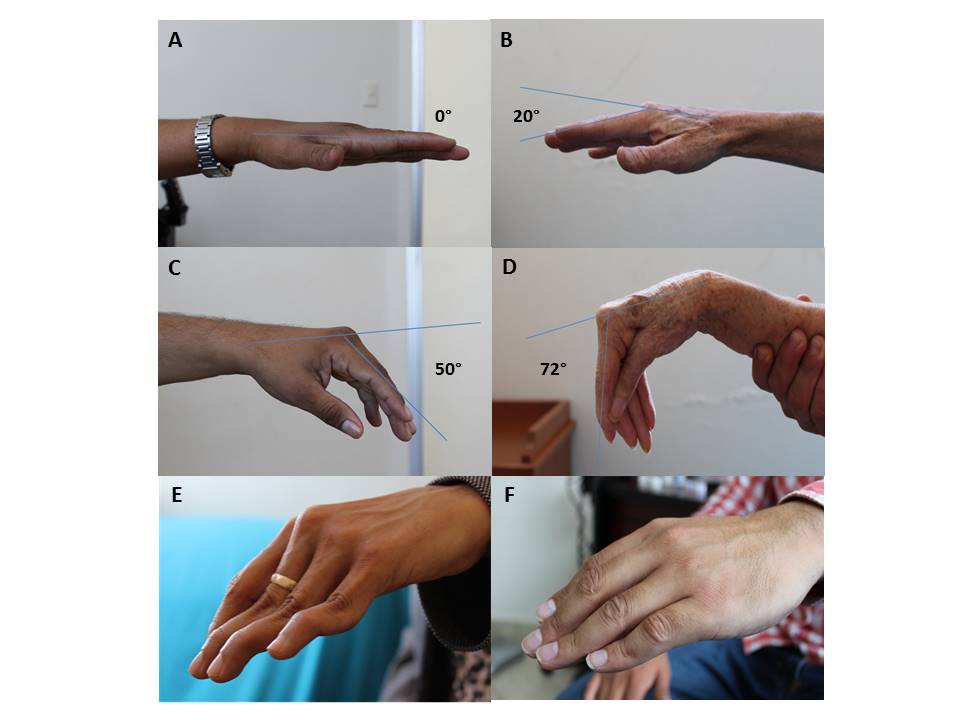
Method: Methods: We evaluated 104 hands of 52 consecutive patients with PD by high resolution photographs taken from the radial aspect of each hand; the degree of flexion of the 2nd metacarpophalangeal (MCP) joint was measured by software. The presence of classical striatal hand deformity (CSHD) was also evaluated, defined as MCP flexion, proximal interphalangeal joint extension and distal interphalangeal joint flexion.
Results: Results: Patients with PD had a mean age of 63.3 ± 12.7 years and 29 (56%) were males. The degree of MCP joint flexion (figure A-D) in both hands showed moderate correlation with the MDS-UPDRS-III motor score (r=0.518, P<0.001); mainly related to ipsilateral rigidity and ipsilateral bradykinesia scores; and fair correlation with the Hoehn-Yahr stage. A CSHD (figure E and F) only correlated with a younger age at onset of PD (P=0.049). These hand deformities were not markers of dyskinesia, levodopa-dose or cognitive dysfunction.
Conclusion: Conclusions: Hand abnormalities are common in patients with PD and consist mainly in mild to moderate degree of MCP joint flexion that correlates with the severity of ipsilateral rigidity and bradykinesia. CSHD is much less common, the fact that presents in individuals having an earlier onset of PD, and lacks correlation with other motor symptoms suggesting that these abnormalities are not necessarily a continuum and may represent two different phenomena.
References: [1] Charcot JM. Lectures on the diseases of the nervous system, lecture V. London: New Sydenham Society; 1877. 140–147 p. [2] Gowers WR. A manual of diseases of the nervous system. Philadelphia: P Blakiston, Son & Co; 1888. 1003-1004 p. [3] Jankovic J. Dystonia and other deformities in Parkinson’s disease. J Neurol Sci 2005;239:1-3. [4] Baizabal-Carvallo JF, Alonso-Juarez M, Fekete R. The frequency and diagnostic accuracy of hand deformities in Parkinson´s disease. J Neural Transm (Vienna) 2018;125: 1813-1817. [5] Spagnolo F, Fichera M, Bucello S, Houdayer E, Baroncini D, Sarro L, Leopizzi E, Impellizzeri M, Martinelli V, Leocani L, Comi G, Volonté MA. Striatal hand in Parkinson’s disease: the re-evaluation of an old clinical sign. J Neurol 2014;261:117-220. [6] Ashour R, Tintner R, Jankovic J. Striatal deformities of the hand and foot in Parkinson’s disease. Lancet Neurol 2005;4:423-431. [7] Ashour R, Jankovic J. Joint and skeletal deformities in Parkinson’s disease, multiple system atrophy, and progressive supranuclear palsy. Mov Disord 2006;21:1856-1863. [8] Gortvai P. Deformities of the hands and feet in Parkinsonism and their reversibility by operation. J Neurol Neurosurg Psychiatry 1963;26:33–36.
To cite this abstract in AMA style:
JF. Baizabal-Carvallo, M. Alonso-Juarez, R. Fekete. Clinical Associations of Hand Deformities in Parkinson´s Disease [abstract]. Mov Disord. 2019; 34 (suppl 2). https://www.mdsabstracts.org/abstract/clinical-associations-of-hand-deformities-in-parkinsons-disease/. Accessed April 2, 2025.« Back to 2019 International Congress
MDS Abstracts - https://www.mdsabstracts.org/abstract/clinical-associations-of-hand-deformities-in-parkinsons-disease/