Session Information
Date: Saturday, October 6, 2018
Session Title: Pathophysiology (Other Movement Disorders)
Session Time: 1:45pm-3:15pm
Location: Hall 3FG
Objective: Investigate Woodhouse-Sakati syndrome through analysis of multimodal evoked potentials at various clinical stages, to assess their possible role as an aid in determining the underlining pathophysiology of the disease.
Background: Woodhouse-Sakati syndrome (WSS) is a rare autosomal recessive multi-systemic disorder, characterized by Hypogonadism, Alopecia, Diabetes Mellitus, sensorineural hearing loss (SNHL) and Extrapyramidal Syndrome. It is caused by homozygous pathogenic variants in DCAF17 gene. The disease is characterized by a progressive nature, manifested through expansion of neurologic involvement, with large proportion of patients developing variable degree of white matter changes on brain MRIs. WSS is hypothesized to be of a demyelinating pathogenesis, but it remains of unclear process.
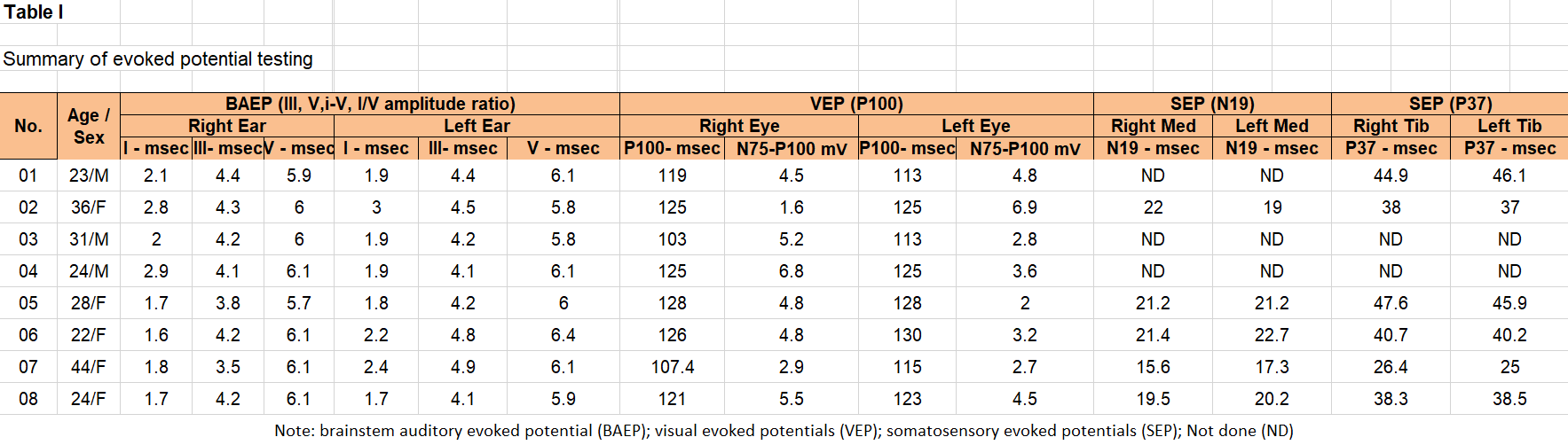
Methods: Evoked potential analysis of eight patients with clinically and genetically confirmed diagnosis of WSS. All patients underwent brainstem auditory evoked potential (BAEP) and visual evoked potentials (VEP). Six patients underwent somatosensory evoked potentials (SEP) in upper and lower limbs (UL, LL).
Results: BAEP was recorded for all patients, and all showed normal wave latencies, interpeak latency and wave V amplitude. VEP was abnormal in all, despite no clinical manifestation of optic neuropathy. 7 out of these 8-patients showed bilateral abnormal VEPs, with only one showing a unilateral abnormal study. Abnormalities were of a prolonged P100 latency, exceeding 111 ms (Normal: 101.5 +/- 9,2 ms), along with abnormal N75 broad morphology and low amplitude (Normal: 704 +/- 2.8 uV). Tibial SEP was done for 6 patients, with 2 patients showing an abnormal prolongation in P37 latency and amplitude. One patients, who was manifested clinically with weakness, showed absent tibial SEP response, with otherwise preserved peripheral component both at the popliteal fossa and N22. Median SEP was conducted in 5 patients, 2 of which showed prolonged N19 cortical response with mildly prolonged N13-N19 inter-peak latency above the lab mean +/- 2 SD.
Conclusions: Evoked potentials analysis in WSS showed variable abnormalities, noted mainly in visual evoked potential studies. This is noted to be subclinical, bilateral in the majority, and the rare finding of a unilateral abnormality likely reflects an ongoing, progressive demyelination. Normal BAEP in the setting of SNHL might indicate involvement of the proximal auditory network above the midbrain, which is also the case in abnormal SEP studies that points to a subcortical pathology. Further studies for better understanding of the disease pathophysiology is required.
References: 1. Bohlega SA, Alkuraya FS. Woodhouse-Sakati Syndrome. In: Adam MP, Ardinger HH, Pagon RA, et al., editors. GeneReviews®. Seattle: University of Washington; 2016:1993-2018. 2. Al-Semari A1, Bohlega S. Autosomal-recessive syndrome with alopecia, hypogonadism, progressive extra-pyramidal disorder, white matter disease, sensory neural deafness, diabetes mellitus, and low IGF1. Am J Med Genet A. 2007 Jan 15;143A(2):149-60. 3. Alazami AM, Schneider SA, Bonneau D, et al. C2orf37 mutational spectrum in Woodhouse-Sakati syndrome patients. Clin Genet 2010;78:585–590.
To cite this abstract in AMA style:
A.H. Abusrair, I. AlHamoud, S. Bohlega. Multimodal evoked potential analysis in Woodhouse-Sakati Syndrome [abstract]. Mov Disord. 2018; 33 (suppl 2). https://www.mdsabstracts.org/abstract/multimodal-evoked-potential-analysis-in-woodhouse-sakati-syndrome/. Accessed June 30, 2026.« Back to 2018 International Congress
MDS Abstracts - https://www.mdsabstracts.org/abstract/multimodal-evoked-potential-analysis-in-woodhouse-sakati-syndrome/