Session Information
Date: Saturday, October 6, 2018
Session Title: Neuroimaging (Non-PD)
Session Time: 1:45pm-3:15pm
Location: Hall 3FG
Objective: To report the presence of caudate nucleus atrophy from early stages of Neuroferritinopathy.
Background: Neuroferritinopathy is a form of neurodegeneration with brain iron accumulation, a rare progressive syndrome that causes movement disorders, and other neurologic deficits. Neuroferritinopathy results in accumulation of iron in basal ganglia due to a mutation in the FTL gene encoding the ferritin light chain. It is characterized by adult-onset of extrapyramidal features like chorea, dystonia, or parkinsonism that are commonly asymmetrical and associated with cognitive impairment.[1] Laboratory tests can show low serum ferritin and brain MRI invariably reveals abnormal deposition of iron in the basal ganglia, as well as cystic changes and necrosis in basal ganglia.[2] The majority of the neuroimaging reports inform the presence of atrophy of the globus pallidus in late stages and correlate it with the severity of this disease, however in our patient the atrophy is located in caudate nucleus and appeared from the beginning of the disease.
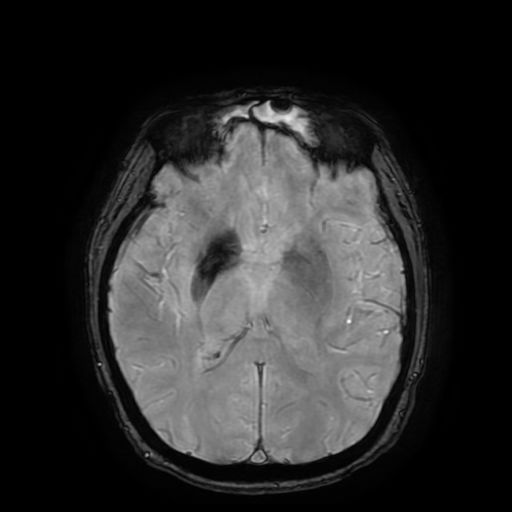
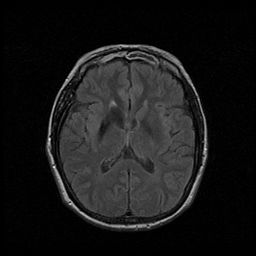
Methods: We present a 47-year-old patient who visits our clinic because she has involuntary movements on the left side of her body, which disappear during sleep and worsen in stressful situations. On examination, these movements correspond to choreoathetosis on her both left extremeties not accompanied by other signs such as tremor, dystonia, parkinsonism or gait alterations. This movement disorder barely interferes on her activities of daily life. Various tests were performed among them: Serum ferritin was 13 μg/L (normal range 15–150 μg/L) and Brain MRI showed irregular cavitation of the right caudate nucleus. Susceptibility weighted imaging showed a band of hypointensity at the periphery of the cavity and at both noncavitated globus pallidus especially in the right side.
Results: During the diagnostic approach we excluded more common causes of choreoathetosis such as Huntington’s disease, pantothenate kinase-associated neurodegeneration, immunological and infectious diseases. Genetic test showed the pathogenic duplication c.460dupA in FTL gene. This information allowed us to reach the diagnosis of Neuroferritinopathy.
Conclusions: We report the presence of atrophy of the caudate nucleus from the beginning of our patient’s symptoms, which raises the possibility that the neuronal loss preceded the onset of the movement disorder. The caudate nucleus atrophy is rarely seen in this disease, because of this we consider it important to report this atypical and early finding in Neuroferritinopathy.
References: 1. Devos, D., Tchofo, P. J., Vuillaume, I., Destée, A., Batey, S., Burn, J., & Chinnery, P. F. (2009). Clinical features and natural history of neuroferritinopathy caused by the 458dupA FTL mutation. Brain, 132(6), e109. http://doi.org/10.1093/brain/awn274. 2. Keogh, M.J., Aribisala, B.S., He, J. et al. J Neurol (2015) 262: 2232. https://doi.org/10.1007/s00415-015-7832-2.
To cite this abstract in AMA style:
G. Alvarez Bravo, J. Fernández Carril, E. Orts Castro. Caudate nucleus atrophy as an early finding of Neuroferritinopathy [abstract]. Mov Disord. 2018; 33 (suppl 2). https://www.mdsabstracts.org/abstract/caudate-nucleus-atrophy-as-an-early-finding-of-neuroferritinopathy/. Accessed March 31, 2025.« Back to 2018 International Congress
MDS Abstracts - https://www.mdsabstracts.org/abstract/caudate-nucleus-atrophy-as-an-early-finding-of-neuroferritinopathy/