Session Information
Date: Thursday, June 8, 2017
Session Title: Other
Session Time: 1:15pm-2:45pm
Location: Exhibit Hall C
Objective: 1.present unusual and rare clinical presentations in the disease spectrum
2.study Intracranial developmental venous anomalies (DVAs) presentations both clinically and radiologically in Wilson’s disease and their association with the disease
Background: Wilson disease is an AR disorder caused by mutation in the ATP7B gene. Neurological manifestations are largely extrapyramidal. DVAs and Wilson’s disease are both considered rare disorders with varying degrees of neurologic and systemic manifestations; yet the coexistence of the two disorders is considered extremely rare
Methods: case report
Results: I.H male patient 18ys old
+ve consanguinity, family history of hepatic diseases and unexplained deaths
The condition started 5 years ago when patient developed recurrent attacks of epistaxis
7months ago patient complained of Dystonia in both UL & LL with opening jaw dystonia and dystonic tremors in right UL associated with parkinsonian features (hypomimia & bradykinesia) and speech difficulty
2months ago patient started experiencing behavioral and psychiatric manifestations in the form of anxiety, disinhibition, verbal & physical aggression and lack of sleep. patient shows worsening of symptoms over the past 2 months with Tip-Toe gait. The patient also experienced recurrent attacks of loss of consciousness associated with generalized tonic clonic convulsions.
1month ago the patient developed acute right LMNL facial palsy and Bulbar symptoms in the form of dysphagia & chocking attacks
Investigations
·LFT: elevated
·Serum Copper: Low
·Serum Ceruloplasmin: Low
·24hr Urinary Copper: Normal
·Pencillamine challenge test: +ve (2257.5 mg/day)
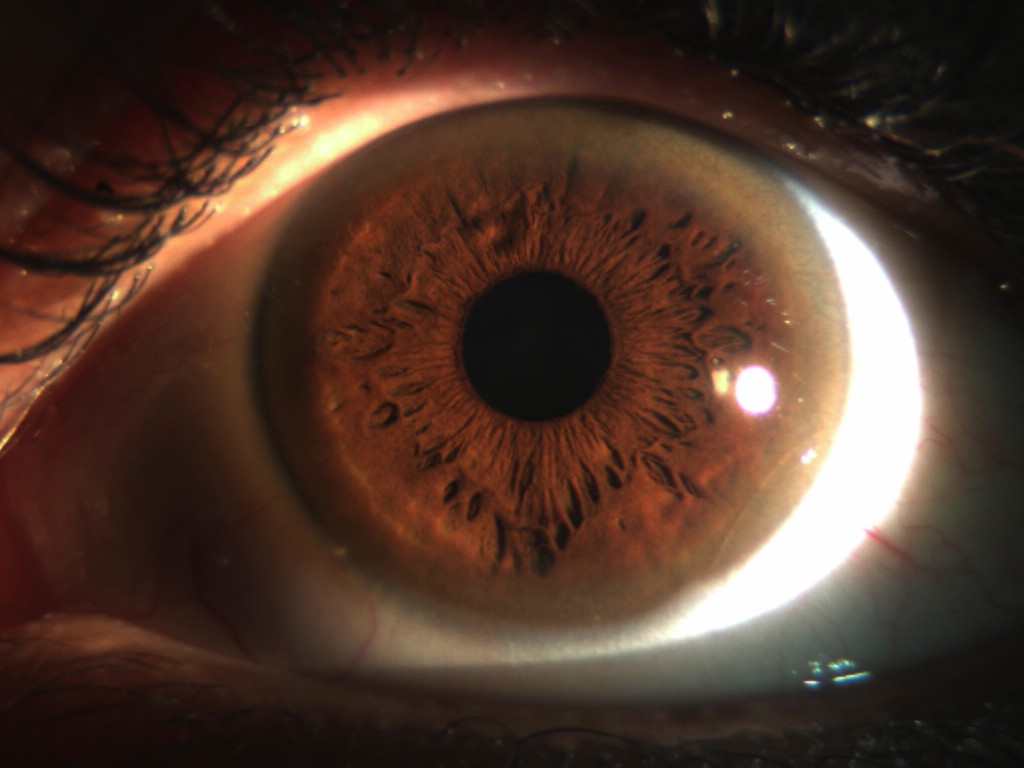
.Slit lamp examination: Kayser–Fleischer rings [Fig.1]
·Abdominal U/S: Liver cirrhosis & splenomegaly
·EEG: Normal
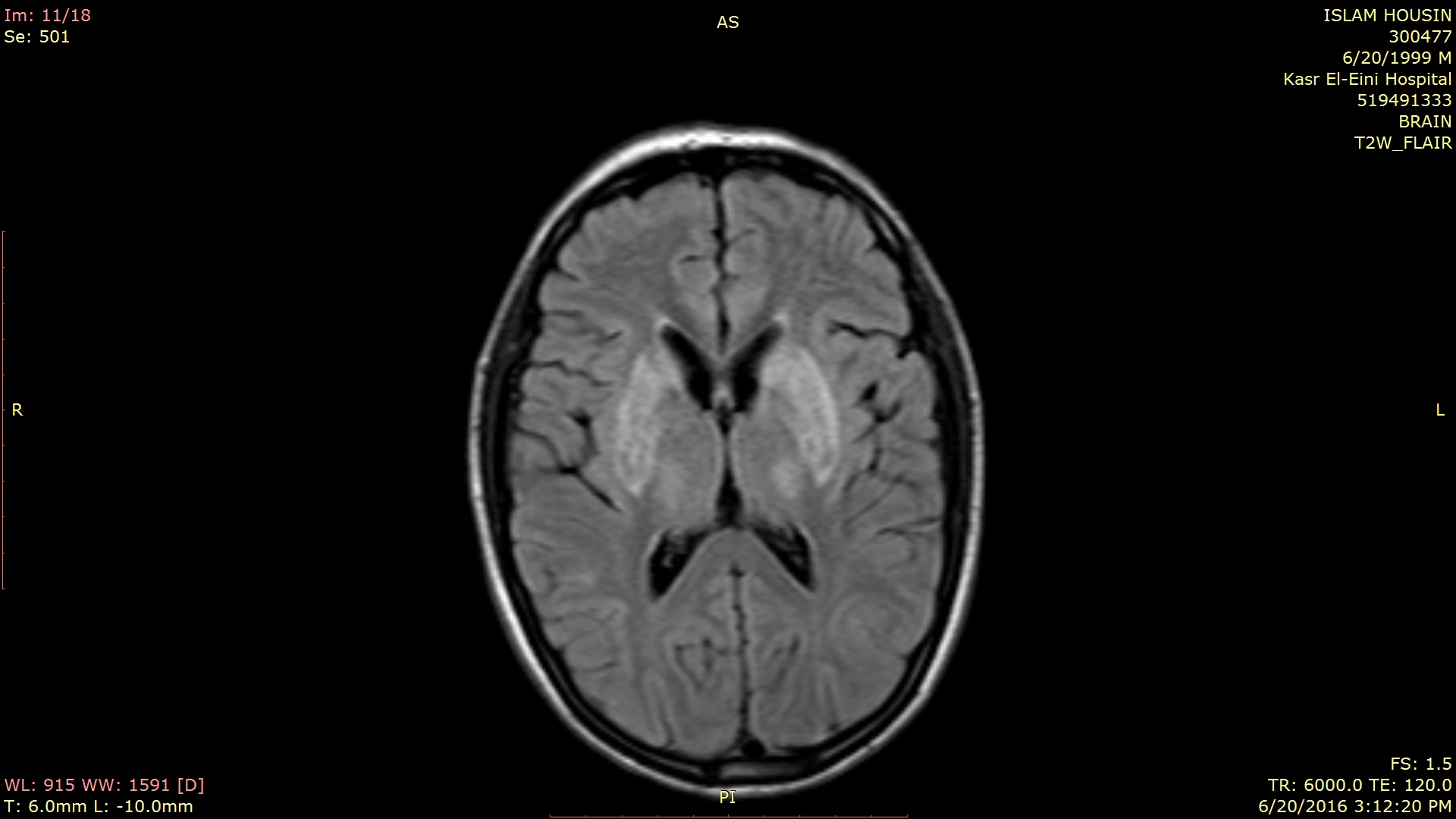
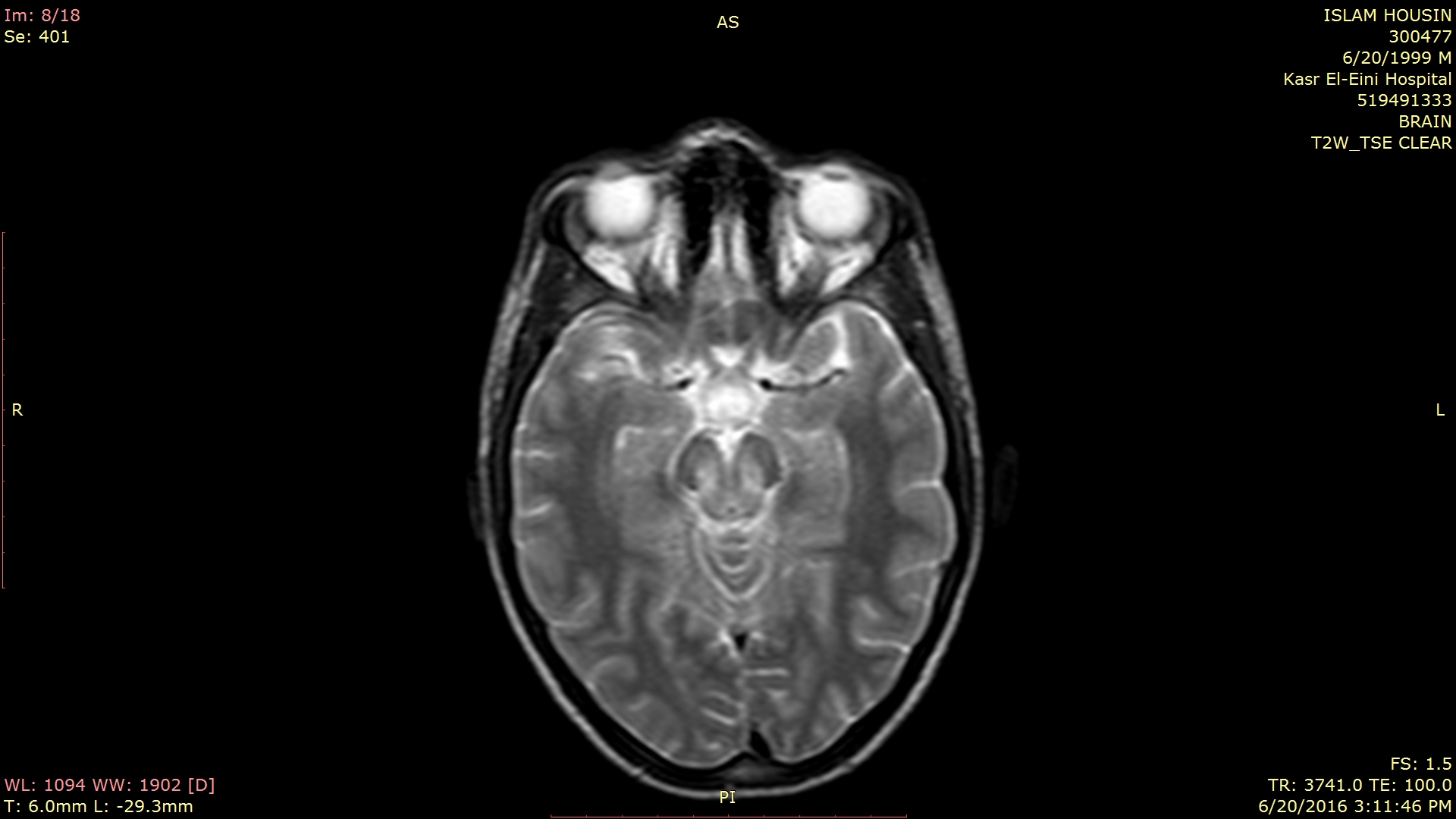
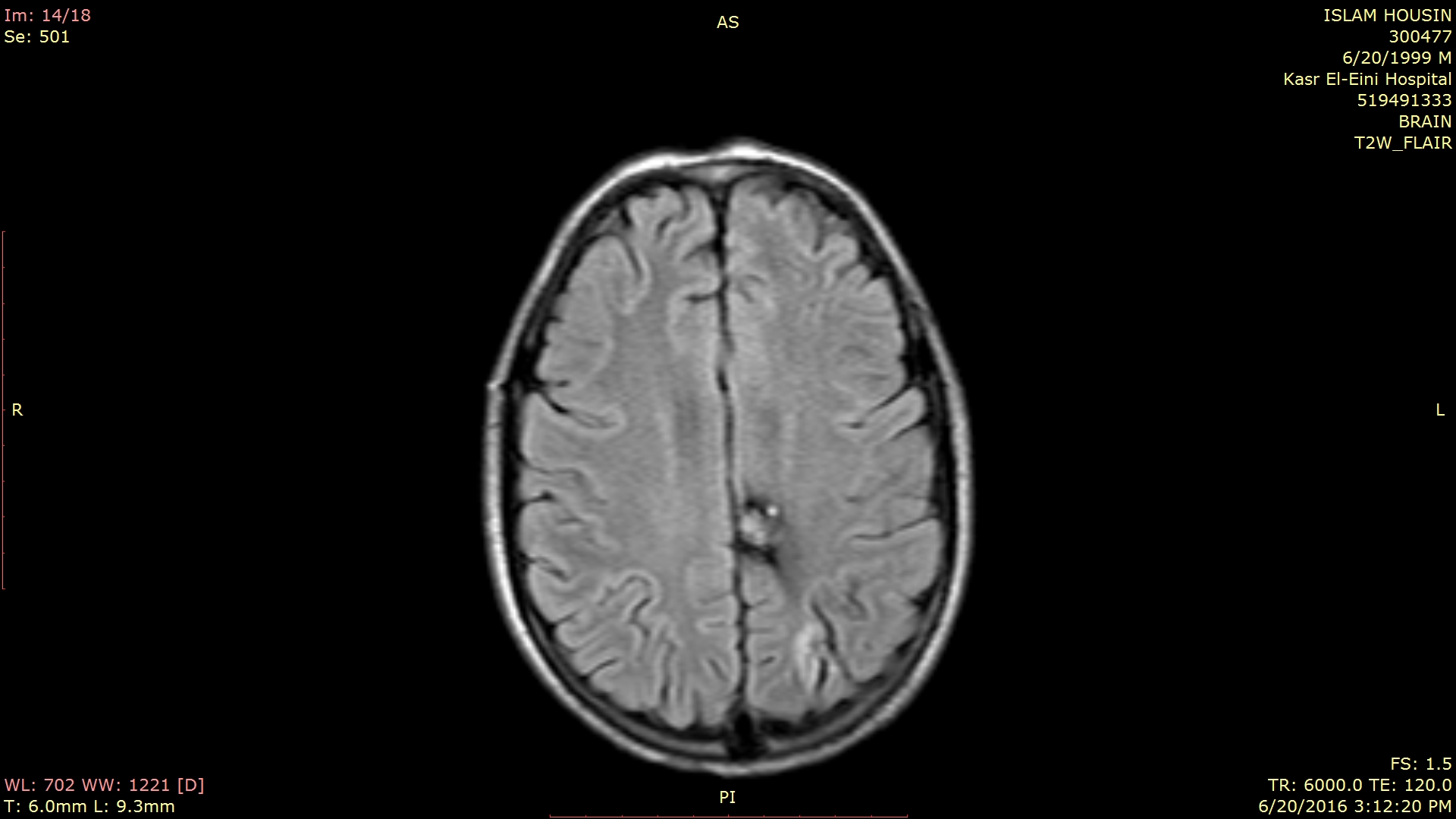
·MRI Brain: Bilateral Basal ganglia, internal capsule, Thalamus and Brain stem T2 hyperintensities + Left parietal venous malformation [Fig.2]
.Genetic Analysis: No mutation detected

Conclusions: 1.Wilson’s disease has very wide spectrum of clinical presentations including rare presentations as epilepsy & cranial nerves affection
2.Epilepsy can occur with either Wilson disease or DVAs; however, the management of coexisting cases may not differ from the management of each disorder individually
3.Pencillamine challenge test can help in diagnosis of Wilson’s disease patients with normal 24hr. urinary copper and further studies on adults is encouraged
References: 1. Ronald F. Pfeiffer: Wilson’s Disease. SEMINARS IN NEUROLOGY/VOLUME 27, NUMBER 2, 2007.
2. Ammar Alobaidy, Faisal Alazri, P.C. Jacob and Jamila H. Al-Kalbani: Presentation of Epilepsy in a Patient with Wilson’s Disease and Developmental Venous Anomaly (Venous Angioma) in the Brain. Sultan Qaboos Univ Med J. 2012 Nov; 12(4): 503–507.
To cite this abstract in AMA style:
W. Ezzat, A. Mohamed. Epilepsy and Cranial nerve affection in a Patient with Wilson’s disease and Intracranial developmental venous anomaly; A Case Report [abstract]. Mov Disord. 2017; 32 (suppl 2). https://www.mdsabstracts.org/abstract/epilepsy-and-cranial-nerve-affection-in-a-patient-with-wilsons-disease-and-intracranial-developmental-venous-anomaly-a-case-report/. Accessed March 31, 2025.« Back to 2017 International Congress
MDS Abstracts - https://www.mdsabstracts.org/abstract/epilepsy-and-cranial-nerve-affection-in-a-patient-with-wilsons-disease-and-intracranial-developmental-venous-anomaly-a-case-report/