Session Information
Date: Wednesday, June 7, 2017
Session Title: Neurophysiology (Non-PD)
Session Time: 1:15pm-2:45pm
Location: Exhibit Hall C
Objective:
To evaluate R2 Blink Reflex Recovery Cycle (BRRC) in patients with Progressive Supranuclear Palsy (PSP) and CorticoBasal Degeneration (CBD) and to determine its diagnostic sensitivity, specificity, Positive Predictive Value (PPV) and Negative Predictive Value (NPV) in differentiating PSP from CBD.
Background: PSP and CBD are rapidly progressive neurodegenerative disorders, clinically featured by parkinsonism and additional debilitating symptoms. Phenotypic spectrum of these disorders, belonging to the group of tauopathies, is wide. The differential diagnosis between PSP and CBD is extremely difficult because of the overlap of clinical features. R2 BRRC is a neurophysiological tool used to evaluate brainstem excitability. R2 BRRC is abnormal in several movement disorders such as Parkinson’s disease1 and dystonia2.
Methods:
This is a double-blind prospective case-control study. Patients affected by PSP and CBD were consecutively enrolled, according to the currently accepted diagnostic criteria. Patients underwent clinical (Hoehn&Yahr-stage, UPDRS-ME) and neurophysiological (R2 BRRC) assessments. R2 BRRC was performed at interstimulus intervals (ISIs) of 100-150-200-300-400-500-750 ms and it was measured as percentage of R2 amplitude ratio between conditioned and unconditioned response.
Results:
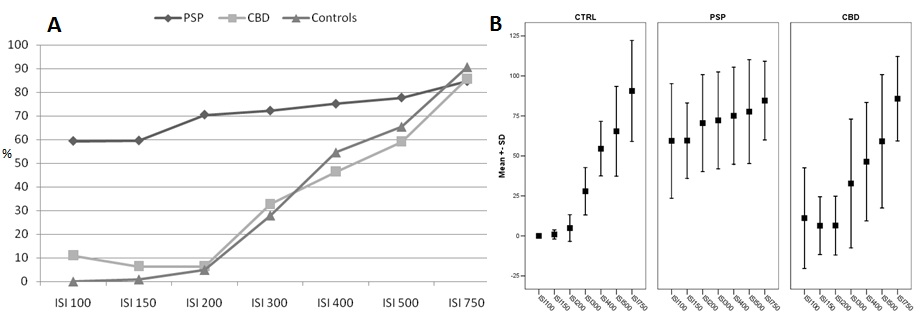
Thirty subjects were enrolled: 12 PSP and 8 CBD patients and 10 healthy controls. Eleven of 12 PSP patients and one of 8 CBD patients showed an early R2 BRRC. A significantly different amplitude of R2 response was observed at ISIs of 100-150-200-300 ms between PSP and CBD patients (p=0.006, p<0.00001, p<0.00001 and p=0.02 respectively) and also between PSP and healthy controls (p<0.00001, p<0.00001, p<0.00001 and p=0.0004 respectively); no statistically significant differences were found between CBD and control subjects [figure1]. An early R2 BRRC differentiated PSP from CBD patients with a sensitivity and a specificity of 87.5% and 91.7% respectively; PPV and NPV were 91.7% and 87.5% respectively.
Conclusions: Despite both diseases belong to a common neuropathological entity, peculiar characteristics can be focused on to distinguish the two disorders. The predominant brainstem tau aggregates distribution in PSP, in contrast with the involvement of neocortex in CBD, could explain the brainstem disinhibition observed in PSP patients. R2 BRRC might be considered a useful tool in differentiating PSP from CBD.
References: 1) Kimura J. Disorder of interneurons in Parkinsonism. The orbicularis oculi reflex to paired stimuli. Brain 1973; 96: 87-96. 2) Berardelli A, Rothwell JC, Day BL, et al. Pathophysiology of blepharospasm and oromandibular dystonia. Brain 1985; 108: 593-608.
To cite this abstract in AMA style:
G. Sciacca, A. Nicoletti, G. Mostile, A. Luca, L. Raciti, V. Dibilio, F. Le Pira, M. Zappia. Blink reflex recovery cycle to differentiate Progressive Supranuclear Palsy from Corticobasal Degeneration [abstract]. Mov Disord. 2017; 32 (suppl 2). https://www.mdsabstracts.org/abstract/blink-reflex-recovery-cycle-to-differentiate-progressive-supranuclear-palsy-from-corticobasal-degeneration/. Accessed April 2, 2026.« Back to 2017 International Congress
MDS Abstracts - https://www.mdsabstracts.org/abstract/blink-reflex-recovery-cycle-to-differentiate-progressive-supranuclear-palsy-from-corticobasal-degeneration/