Session Information
Date: Tuesday, June 6, 2017
Session Title: Drug-Induced Movement Disorders
Session Time: 1:45pm-3:15pm
Location: Exhibit Hall C
Objective: To describe an unusual cause of rhabdomyolysis in patient with advanced Parkinson’s disease (PD) treated with levodopa.
Background: Rhabdomyolysis is a serious and life-threatening condition causing 10% mortality rate. Rhabdomyolysis associated with levodopa-induced dyskinesia (LID) is extremely rare and can potentially be the cause of death in patient with PD.
Methods: case report and literature review
Results: A 64-year-old man was diagnosed PD 7 years ago and has had motor complications including diphasic dyskinesia and wearing-off, for 2 years. The patient currently took levodopa/benzeraside (LB) 650 mg/day, entacapone 500 mg/day, piribedil 150 mg/day and benzhexol 2 mg/day.
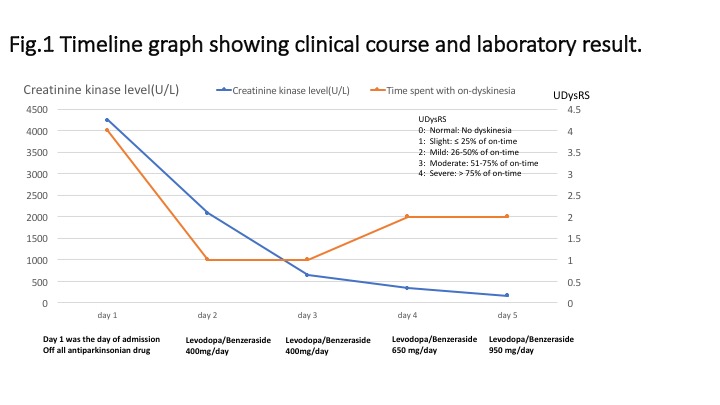
2 days prior to admission, the patient was experienced more wearing off then he shortened the time to take LB every meal. Subsequently, he was suffered from severe generalized dyskinesia which prevented him from normal daily activities. The patient was admitted to our hospital for adjusting medications. On admission, his vital signs were normal (T 37.5 °C, pulse 78 /min, BP 113/75 mmHg). Neurological examinations showed severe dyskinesia involving all extremities, neck, and trunk accompanied with profuse whole body sweating. Bradykinesia was observed on his arms and feet bilaterally; however, rigidity and tremor were not detected. Complete blood counts was normal. Creatinine, BUN, potassium, AST, and ALT slightly increased. Surprisingly, creatinine kinase (CPK) markedly increased (4,246 U/L). Urinalysis did not show evidence of myoglobinuria. Rhabdomyolysis associated with LID was diagnosed.
The patient was hydrated with intravenous isotonic saline. Diazepam 10 mg was given intravenously and all anti-parkinsonian medications were stopped. Few days later, dyskinesia continuously improved. On day 5, his blood tests showed mark improvement. CPK was decreased to 170 U/L. Levodopa was re-challenged to control his parkinsonian symptoms. On discharge, medication was adjusted to LB 950 mg/day without other anti-parkinsonian medications. To control severe motor complications, the patient was scheduled for performing deep brain stimulation surgery.
Conclusions: Despite of parkinsonism-hyperpyrexia syndrome, rhabdomyolysis associated with LID is another potential life-threatening complication in patient with PD. Awareness, early detection and early treatment can minimize further complications and leads to a favorable outcome.
References: 1.Zutt R, van der Kooi AJ, Linthorst GE, Wanders RJA, de Visser M. Rhabdomyolysis: review of the literature. Neuromuscul Disord. 2014;24:651-9.
2.Lyoo CH, Lee MS. Rhabdomyolysis induced by severe levodopa induced dyskinesia in a patient with Parkinson’s disease. J Neurol 2011;258:1893–4
To cite this abstract in AMA style:
Y. Pitakpatapee, C. Satukijchai, P. Srivanitchapoom. An Unusual Cause of Rhabdomyolysis in Parkinson’s disease [abstract]. Mov Disord. 2017; 32 (suppl 2). https://www.mdsabstracts.org/abstract/an-unusual-cause-of-rhabdomyolysis-in-parkinsons-disease/. Accessed April 2, 2025.« Back to 2017 International Congress
MDS Abstracts - https://www.mdsabstracts.org/abstract/an-unusual-cause-of-rhabdomyolysis-in-parkinsons-disease/