Session Information
Date: Wednesday, June 22, 2016
Session Title: Choreas (non-Huntington's disease)
Session Time: 12:00pm-1:30pm
Location: Exhibit Hall located in Hall B, Level 2
Objective: To describe the natural history and imaging findings in a case of untreated diabetic striatopathy.
Background: Diabetic striatopathy (DS) is a rare movement disorder characterized by unilateral hemichorea/hemiballismus with characteristic MRI findings of T1 hyperintensity of the contralateral basal ganglia secondary to non-ketotic hyperglycemia or diabetic ketoacidosis. The pathophysiology is thought to involve blood-brain barrier dysfunction, obliterative vasculopathy with prominent angiogenesis, and ultimately the selective depletion of inhibitory GABA-ergic neurons in the striatum. Typically, with prompt normalization of blood glucose and related metabolic derangements, both symptoms and imaging abnormalities resolve within days to weeks.
Methods: Case report.
Results: A 57 year old woman with poorly controlled type 2 diabetes mellitus presented to our movement disorders clinic with chronic abnormal movements of the left hand, wrist, and forearm of approximately four years duration. Onset was acute and the movements initially consisted of ballistic flexion/extension movements of the wrist and elbow. Gradually they evolved to nearly continuous choreoathetoid abduction/adduction movements of the thumb, flexion/extension motion of the fingers, and some rotatory movements of the wrist. MRI performed about 6 months after symptom onset showed anatomically demarcated T1 hyperintense/ T2 hypointense/GRE-positive basal ganglia signal (Fig. 1A). Trials of levodopa, ropinirole, and trihexyphenidyl did not result in significant improvement; clonazepam reduced the amplitude and frequency of the movements modestly. Treatment with olanzapine in our clinic has been highly effective. Follow up imaging demonstrated resolution of the T1 hyperintensity but severe atrophy of the affected caudate head (Fig 1B). 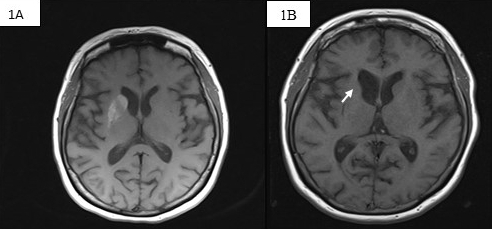
Conclusions: The usual natural history of DS suggests that the characteristic movements and imaging usually resolve over a short time with strict glycemic control. Unfortunately our patient’s DM remained uncontrolled, which apparently resulted in ongoing pathology with permanent chorea and atrophy of the caudate head. To our knowledge this is the first reported case describing the natural history of diabetic striatopathy in which the underlying metabolic abnormality is left uncorrected, and emphasizes the importance of early recognition and management of movement disorders associated with metabolic abnormalities.
To cite this abstract in AMA style:
B. Krishnaiah, E. Lucassen, M.C. Stahl. Persistent hemichorea and caudate atrophy in untreated diabetic striatopathy [abstract]. Mov Disord. 2016; 31 (suppl 2). https://www.mdsabstracts.org/abstract/persistent-hemichorea-and-caudate-atrophy-in-untreated-diabetic-striatopathy/. Accessed April 1, 2025.« Back to 2016 International Congress
MDS Abstracts - https://www.mdsabstracts.org/abstract/persistent-hemichorea-and-caudate-atrophy-in-untreated-diabetic-striatopathy/